Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG.
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order. Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 84-50-77
Age: 53
Gender: Male
Length of Stay: 6 Days
Service Type: Inpatient
Discharge Status: To Home
Diagnosis/Procedure: Atherosclerosis Coronary Arteries.
Unstable Angina.
Double Coronary Artery Bypass.
DISCHARGE SUMMARY
PATIENT: JED INPATIENT
RECORD NUMBER: 84-50-77
ADMITTED: 06-15-XX
DISCHARGED: 06-20-XX
PHYSICIAN: DR. ALEX, M.D.
DIAGNOSIS: Atherosclerosis coronary arteries with chronic total occlusion.
Unstable angina.
Congestive heart failure, combined systolic and diastolic, chronic.
PROCEDURE: Coronary artery bypass graft x 2.
HISTORY OF THE PRESENT ILLNESS: The patient is a 53-year-old male who presents with unstable angina of two hours duration in the emergency room. The patient was noted to be in congestive heart failure with impending probable infarction. The patient was admitted directly to the CCU.
LABORATORY DATA: Glucose 106, BUN 11, creatinine 1.1, liver function tests are all normal, albumin 4.2, sodium 141, potassium 4.8, cholesterol 166, triglycerides 122, iron 82. White count 6900, hemoglobin 17.2, MCV 95, platelets 136,000.
HOSPITAL COURSE: The patient was admitted to the CCU at the hospital. Workup revealed the patient to have atherosclerosis of the coronary arteries, unstable angina, with congestive heart failure in need of a double bypass. The patient underwent coronary artery bypass with resolution of angina. The patient tolerated the procedure well and was responding well to the CABG postsurgical clinical pathway. The patient was sitting up on the night of the surgery and standing the next morning. The patient progressed from that point and is very motivated to recover and manage his health. Patient was also treated for the congestive heart failure in the hospital and will be on medication for this diagnosis daily.
DISCHARGE PLANS: The patient is to follow up with me in the office in one week or sooner if needed. Prescription for Capoten 12.5 mg 1½ tablets q 12 hours and Lasix 1 mg q daily.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 06-21- xx 8567
HISTORY and PHYSICAL
PATIENT: JED INPATIENT
RECORD NUMBER: 84-50-77
ADMITTED: 06-15-XX
DISCHARGED: 06-20-XX
PHYSICIAN: DR. ALEX, M.D.
CHIEF COMPLAINT: Unstable angina.
HISTORY OF PRESENT ILLNESS: The patient is a 53-year-old male who presents with unstable angina of 2 hours duration in the emergency room. The patient was noted to be in congestive heart failure with impending probable infarction. The patient was admitted directly to the CCU.
ALLERGIES: None known.
MEDICATIONS: None.
SOCIAL HISTORY: The patient is an automotive repair technician. The patient smokes one and a half packs of cigarettes daily for 30 years. Grandfather, paternal, died of myocardial infarction at age 64.
MEDICAL HISTORY: Patient notes chest discomfort, neck discomfort, and arm discomfort typical of pre-infarction/unstable angina on and off for the last 2 months. The patient has also had an upper respiratory infection with productive cough, runny nose, sneezing, in the last month with no symptoms today. He does recall several episodes of epigastric discomfort manifest as a pressure sensation lasting perhaps a day at a time in the past months but states he ignored it and the pressure sensation and discomfort went away.
The patient has no orthopnea, PND, or edema. He has occasional heart racing but no lightheaded spells, near syncope, or syncope. There is no history of hypertension, hyperlipidemia, diabetes, congenital heart disease, rheumatic fever, heart murmur, or MI.
REVIEW OF SYSTEMS:
His general review of systems in detail is unremarkable. His only surgery is minor surgery on his knee. He does not use alcohol at all and never has. He has no GI distress. He denies history of drug abuse, eye problems, cancer liver disease, emphysema, thyroid problems, gout, asthma, hay fever, hives, migraine headaches, TIA's, stroke, deep venous thrombosis, pulmonary embolism, kidney stones, etc.
PHYSICAL EXAMINATION:
GENERAL: BP 140/101, pulse 98, respirations distension.
LUNGS: Clear.
HEART: As previously noted, angina, rapid rate.
ABDOMEN: Unremarkable.
SKIN: Is warm and dry. Temp 97.9.
NECK: Slight jugular venous distension.
EXTREMITIES: There is no peripheral edema.
ASSESSMENT: Unstable angina.
Congestive heart failure, combined systolic and diastolic, chronic.
Heavy, current smoking history.
PLAN: Admit for cardiac workup and possible coronary artery bypass surgery. The risks, alternatives, risks and other options were explained to the patient. The patient wishes to proceed with the bypass surgery if indicated.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 06-15- xx 8567
OPERATIVE REPORT
PATIENT: JED INPATIENT
RECORD NUMBER: 84-50-77
SURGERY DATE: 06-15-XX
DISCHARGED: 06-20-XX
SURGEON: DR. ALEX, M.D.
PREOPERATIVE DIAGNOSIS: 1.Atherosclerosis aoronary arteries with chronic total occlusion.
2. Unstable angina.
3. Congestive heart failure, combined systolic and diastolic, chronic.
POSTOPERATIVE DIAGNOSIS: 1. Atherosclerosis coronary arteries with chronic total occlusion.
2. Unstable angina.
3. Congestive heart failure, combined systolic and diastolic, chronic.
OPERATIVE PROCEDURE: Coronary artery bypass graft x 2 using greater saphenous vein from aorta to right mid coronary artery and distal right coronary artery.
ANESTHESIA: General.
DESCRIPTION: The patient was taken to the operating room and placed on the operating table in a supine position. Patient was adequately anesthetized using general inhalation anesthesia with pulmonary and arterial artery monitoring and sterile prep of the surgical field, a sterile midline sternotomy was performed. The ascending aorta and right atrium was anatomically identified and preparatory purse-string sutures were placed in both the ascending aorta and right atrium. The next step in the procedure was to institute cardiopulmonary bypass with a single, two-stage venous uptake tube. Saphenous vein was harvested from the left leg using the endoscope. The aorta was clamped above the heart. Cardioplegia was affected with cold preserving solution pumped through the coronary arteries to stop the heart. The right coronary artery was identified with anatomical area chosen beyond the diseased portion and a longitudinal incision was cut in it. The proximal part of the vein was trimmed to the same length as the cut in the coronary artery and is cleaned off. Using 6-0 Prolene suture, end-to side anastomosis was created between the right mid coronary artery and the aorta. This was duplicated for the second opening and end-to-side anastomosis was performed from the aorta to the distal right coronary artery. The clamp on the aorta was released and following spontaneous contraction of the heart, cardiopulmonary bypass was discontinued. The patient was observed for a time with stable heart function. Approximation of the pericardium was then performed with hemostasis obtained. Sternum was approximated with surgical stainless steel parasternal wire. Fascia and skin was closed with Vicryl sutures. The patient tolerated the procedure well and was transferred to the recovery room in stable condition.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 06-15- xx 8567
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

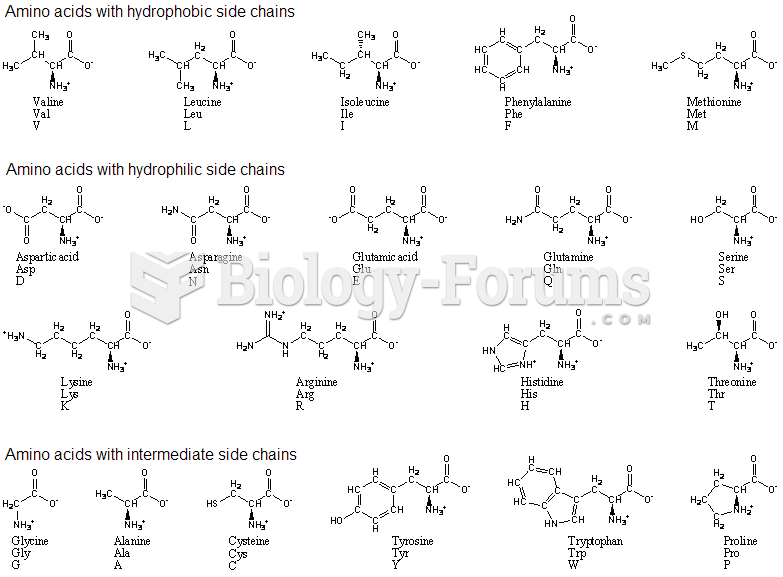 amino acids with single and three code
amino acids with single and three code
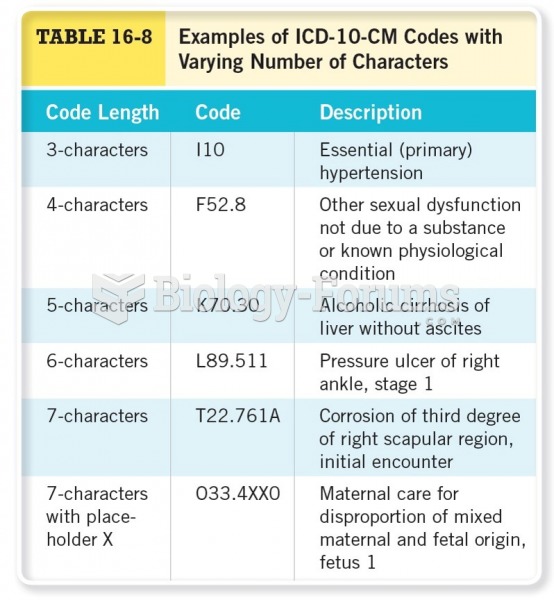 Examples of ICD-10-CM Codes with Varying Numbers of Characters
Examples of ICD-10-CM Codes with Varying Numbers of Characters
 Review Bundling, Add-on Codes, and Quantity Edits
Review Bundling, Add-on Codes, and Quantity Edits
 Compare the Final Code with the Documentation
Compare the Final Code with the Documentation
 Corroded terminals on a waste-spark coil can cause misfire diagnostic trouble codes to be set.
Corroded terminals on a waste-spark coil can cause misfire diagnostic trouble codes to be set.
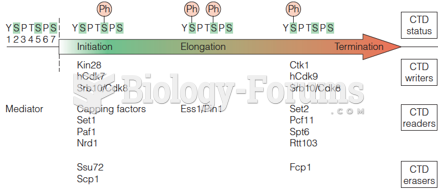 Writers, readers, and erasers of the CTD phosphorylation code
Writers, readers, and erasers of the CTD phosphorylation code