Code the following cases for inpatient facility purposes using ICD-9-CM and ICD-10-CM and PCS codes.
Calculate the MS-DRG .
Identify the Principal vs. Secondary diagnoses and procedures.
Use external cause codes when appropriate.
Do NOT code procedures that are captured by the facility chargemaster.
Secondary diagnoses and procedures do NOT need to be sequenced in any particular order.
Enter "None" when no code is required.
If more than one occurrence of a procedure is required, report the code with "x 2""x 3" etc.
INPATIENT HOSPITAL
Health Record Face Sheet
Record Number: 77-50-77
Age: 76
Gender: Male
Length of Stay: 6 Days
Service Type: Inpatient
Discharge Status: To Home
Diagnosis/Procedure: Hemoptysis
Fiberoptic bronchoscopy with biopsy
DISCHARGE SUMMARY
PATIENT: JARED INPATIENT
RECORD NUMBER: 77-50-77
ADMITTED: 06-15-XX
DISCHARGED: 06-21-XX
PHYSICIAN: DR. ALEX, M.D.
DIAGNOSIS: Hemoptysis.
Hypertension.
Atelectasis.
PROCEDURE: Fiberoptic bronchoscopy x 2 with biopsy.
HISTORY OF THE PRESENT ILLNESS: The patient is a 76-year-old white male admitted to the hospital with hemoptysis. The patient states that approximately three weeks ago, he had the onset of hemoptysis associated with clear sputum. This was not accompanied by chest pain, fever, or change in his chronic mild dyspnea. He did not have any pedal edema, PND, or orthopnea associated with it. He was given prescriptions for Lasix and Erythromycin when a chest x-ray report returned suggestive of possible congestive heart failure and/or pneumonia. He states that since then, his hemoptysis has significantly decreased though it is still present in the mornings. He is having difficulty feeling tired all the time but has not had any difficulty with sleep per se. There is no prior history of pneumonias and no prior history of CHF. He relates that he had an echocardiogram yesterday, results of which are unknown. There is no known TB exposure. The patient was born and raised here in this state.
HOSPITAL COURSE: The patient was admitted and bronchoscopy was performed to evaluate hemoptysis and rule out carcinoma. Left lower lobe was collapsed, probably secondary to the left hemidiaphragm paralysis. There were no other endobronchial lesions. It should be noted that saturation by oximeter was 85% before the start of the procedure and before any sedative mediations were given. On day two of hospitalization, the patient was given another bronchoscopy with biopsies to work up possible atelectasis. Prior to the second bronchoscopy the patient was noted to have multifocal PVCs on the monitor before starting the procedure. The right sided tracheal bronchial tree was characterized by prominent changes of chronic inflammation. This was most impressive in the left lower lobe. The left lower lobe orifice was narrowed by extrinsic compression. The left lower lobe segmental orifices were markedly narrow due to extrinsic compression. Neither the brush nor the transbronchial biopsy forceps could be passed into the posterior or lateral segmental orifices. Endobronchial biopsies, brushings and washings were obtained from the left lower lobe segmental orifices.
DISCHARGE PLANS: The patient was provided home oxygen, prn. Inhaler prescription was provided along with instructions. The patient is to follow up in the office in 2 days.
DR. ALEX, M.D.
Electronically authenticated by Dr. Alex, M.D., 06-21- xx 856
HISTORY AND PHYSICAL
PATIENT: JARED INPATIENT
RECORD NUMBER: 77-50-77
ADMITTED: 06-15-XX
DISCHARGED: 06-21-XX
PHYSICIAN: DR. ALEX, M.D.
HISTORY OF PRESENT ILLNESS: The patient is a 76-year-old white male admitted to the hospital with hemoptysis. The patient states that approximately 3 weeks ago, he had the onset of hemoptysis associated with clear sputum. This was not accompanied by chest pain, fever, or change in his chronic mild dyspnea. He did not have any pedal edema, PND, or orthopnea associated with it either. He was given prescriptions for Lasix and Erythromycin when a chest x-ray report returned suggestive of possible congestive heart failure and/or pneumonia. He states that since then, his hemoptysis has significantly decreased though it is still present in the mornings. He is having difficulty feeling tired all the time but has not had any difficulty with sleep per se. There is no prior history of pneumonias and no prior history of CHF. He relates that he had an echocardiogram yesterday, results of which are unknown. There is no known TB exposure.
CURRENT MEDICATIONS: Cardene 20 mg, 1 tid, Lasix 20 mg, 1 qid.
SOCIAL HISTORY: The patient quit smoking 30 years ago after 30 years of one pack per day. He was an engineer with the railroad for much of his working career. He did some work for a total of about 9 months between 1939 and 1940 in a backroom where there was much asbestos work being done and he feels that it was aerosolized.
PAST MEDICAL HISTORY: He has known of high blood pressure for 2 to 3 years. His only prior surgery was an eye removal after an accident recently.
FAMILY HISTORY: Father died of cancer, one brother died of an MI and another brother died of cancer.
REVIEW OF SYSTEMS: Negative for kidney disease. Patient has known previous heart disease, phlebitis, rheumatic fever, hepatitis, liver disease, or peptic ulcer disease.
PHYSICAL EXAM:
VITAL SIGNS: BP is 180/100 and pulse is 80.
HEENT: Unremarkable with a normal oropharynx.
NECK: Supple without adenopathy or thyromegaly.
CHEST: Has Velcro type rales at the right base. There is dullness where the left lung base should be. There are only a very few rales above that region. There are no wheezes heard after bronchodilator.
ABDOMEN: Soft without tenderness, masses, or hepatosplenomegaly.
EXTREMITIES: Without clubbing, cyanosis or edema.
LABORATORY DATA: Room air blood gas obtained on the third hospital day, pH 7.45, PO2 58, PCO2 38. CBC and serum chemistries were within normal limits.
Spirometry today shows a severe decrease in FVC which is partly related to air trapping. There is at least mild obstruction. There was a 53% improvement in FVC after Atrovent treatment.
Chest x-rays are reviewed from one month ago and today. Those from one month ago showed dense interstitial infiltrate in the right lung predominant in the mid and lower lung region. There is some subsegmental atelectasis at the left base above his elevated left hemidiaphragm. The chest x-ray report from that time notes that this is probably old and was suggested on a previous upper GI. The right hilum, I believe is bulky. The heart is enlarged. Film today shows the vast majority of the infiltrate in the right base has resolved. The right hilum remains bulky in appearance.
IMPRESSION:
1. Hemoptysis. Resolving right lower lobe infiltrate suggest probable pneumonia. There may also be some interstitial lung disease associated with asbestos exposure, as there is persistence of rales on exam. Congestive heart failure. I am concerned; however, about the bulky appearance of the right hilum and that this may have been a post obstructive pneumonia. Furthermore, the hemoptysis is persisting.
2. Chronic obstructive pulmonary disease and restrictive defect secondary to elevated hemidiaphragm. As the patient is only very mildly symptomatic with dyspnea and noticed no symptomatic improvement Atrovent inhaler is prescribed two puffs q 4 hours on a prn basis.
PLAN: Bronchoscopy rule out endobronchial neoplasm.
DR. ALEX, M.D.
Electronically signed by Dr. Alex, 06-15-xx, 3345
OPERATIVE REPORT
PATIENT: JARED INPATIENT
RECORD NUMBER: 77-50-77
DATE OF SURGERY: 06-15-XX
SURGEON: DR. ALEX, M.D.
PREOPERATIVE DIAGNOSIS: Hemoptysis.
POSTOPERATIVE DIAGNOSIS: 1. Hemoptysis, probably secondary to pneumonia.
2. Possible chronic hypoxemia.
OPERATIVE PROCEDURE: Fiberoptic bronchoscopy.
INDICATION: This 76-year-old white male had the onset of hemoptysis approximately 3-4 weeks ago. A chest x-ray revealed a right lower lobe infiltrate, left diaphragm paralysis, and signs of possible congestive heart failure. He was started on Erythromycin and Lasix with subsequent gradual tapering in the amount of hemoptysis. For the week prior to today, he has had only one episode. The chest x-ray showed interval improvement but the right hilum was felt to be enlarged. He is a former smoker and because the hemoptysis persisted for such a long period of time bronchoscopy was indicated to rule out endobronchial abnormality.
DESCRIPTION: The P20 fiberoptic bronchoscope was passed via nasal approach. The upper airway was normal. The tracheal bronchial tree was remarkable for quite prominent diffuse changes of chronic inflammation with linear striations. The segmental orifices of the left lower lobe were collapsed, probably secondary to the left hemidiaphragm paralysis. There were no other endobronchial lesions. It should be noted that saturation by oximeter was 85% before the start of the procedure and before any sedative mediations were given.
IMPRESSION:
1. Hemoptysis, probably secondary to pneumonia.
2. Possible chronic hypoxemia.
DR. ALEX, M.D.
Electronically signed by Dr. Alex, 06-15-xx, 3345
OPERATIVE REPORT
PATIENT: JARED INPATIENT
RECORD NUMBER: 77-50-77
DATE OF SURGERY: 06-16-XX
SURGEON: DR. ALEX, M.D.
PREOPERATIVE DIAGNOSIS: Left lower lobe atelectasis.
POSTOPERATIVE DIAGNOSIS: Left lower lobe atelectasis with abnormal endobronchial findings as described.
OPERATIVE PROCEDURE: Fiberoptic bronchoscopy with endobronchial biopsies, brushings and washings left lower lobe segmental
INDICATIONS: This 76-year-old white male was admitted with hemoptysis and is now being evaluated for atelectasis. CT scan of the chest showed some left lower lobe atelectasis. Follow up CT scan of the chest showed decrease in the size of the left lower lobe scan of the chest showed decrease in the size of the left lower lobe atelectasis which was felt to be possibly related to an elevated left hemi-diaphragm. Recent repeat follow up CT scan of the chest showed increase in the amount of left lower lobe atelectasis and an apparent pleural effusion associated with it. The patient has not had any new symptoms. He is felt to have probable asbestosis by his exposure history and finding pleural plaques and interstitial fibrosis on chest x-ray and CT scan.
DESCRIPTION: The patient was noted to have multifocal PVCs on the monitor before starting the procedure and was therefore pre-medicated with 75 mg of Lidocaine IV. He was also given 0.5 mg of Versed IV as well as Robinul 0.3 mg IM. A P-20 fiberoptic bronchoscope was passed via nasal approach. The upper airway was felt to be within normal limits. The right sided tracheal bronchial tree was characterized by prominent changes of chronic inflammation. This was most impressive in the left lower lobe. The left lower lobe orifice was narrowed by extrinsic compression. The left lower lobe segmental orifices were markedly narrow due to extrinsic compression. Neither the brush nor the transbronchial biopsy forceps could be passed into the posterior or lateral segmental orifices. Endobronchial biopsies, brushings and washings were obtained from the left lower lobe segmental orifices. These areas were quite friable. The patient tolerated the procedure without apparent difficulty and only occasional PVCs were noted during the procedure. Saturation on room air post procedure is 91%.
PATHOLOGY REPORT RESULTS: Bronchial mucosal fragments, left lower lobe, showing no diagnostic features.
DR. ALEX, M.D.
Electronically signed by Dr. Alex, 06-16-xx, 3345
ICD-9-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-9-CM procedure code(s): PPx_____________________
SPx_____________________
ICD-10-CM diagnosis code(s): PDx_____________________
SDx _____________________
ICD-10-PCS procedure code(s): PPx_____________________
SPx_____________________
MS-DRG: _____________________

 An elephant can use its trunk for a variety of purposes. This one is wiping its eye.
An elephant can use its trunk for a variety of purposes. This one is wiping its eye.
 These older adults are participating in an exercise class at their assisted-living facility
These older adults are participating in an exercise class at their assisted-living facility
 An extended care facility.
An extended care facility.
 Compare the Final Code with the Documentation
Compare the Final Code with the Documentation
 A plastic MAP sensor used for training purposes showing the electronic circuit board and electrical ...
A plastic MAP sensor used for training purposes showing the electronic circuit board and electrical ...
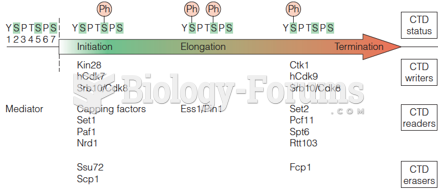 Writers, readers, and erasers of the CTD phosphorylation code
Writers, readers, and erasers of the CTD phosphorylation code