This topic contains a solution. Click here to go to the answer
|
|
|

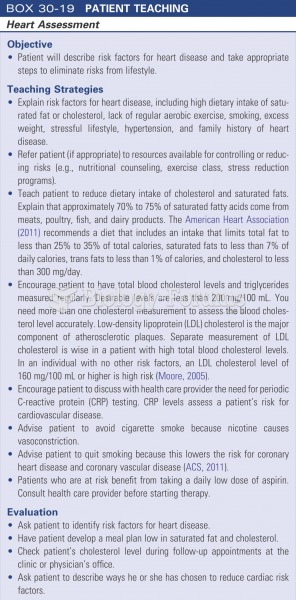 Patient teaching: heart assessment
Patient teaching: heart assessment
 It is important to act concerned when a patient is upset.
It is important to act concerned when a patient is upset.
 Positioning the Patient in the Prone Position
Positioning the Patient in the Prone Position
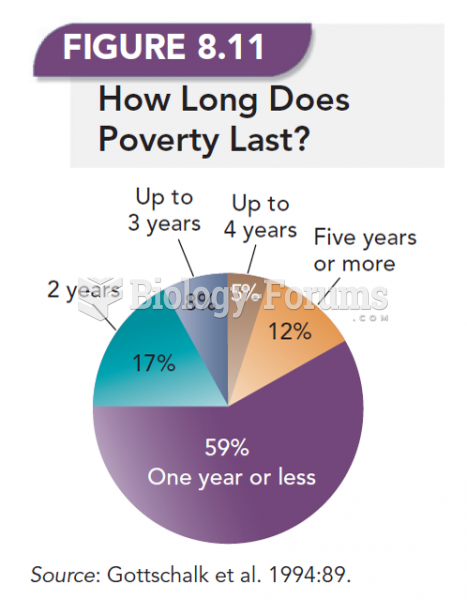 How Long Does Poverty Last?
How Long Does Poverty Last?
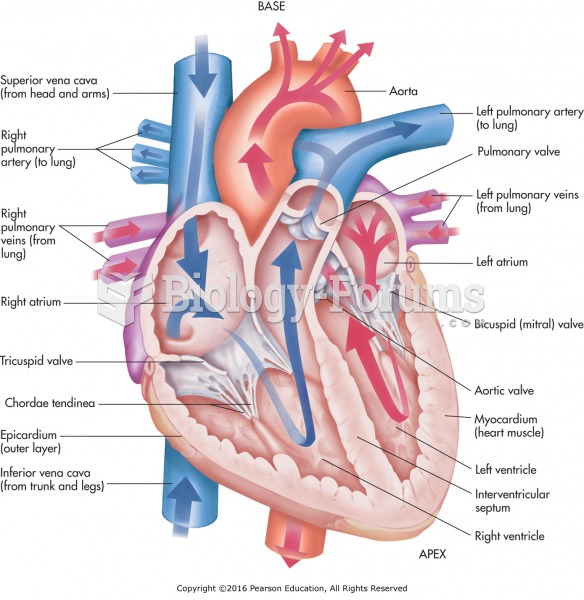 Anatomy of the heart. Remember: It is labeled right and left based on the patient’s perspective.
Anatomy of the heart. Remember: It is labeled right and left based on the patient’s perspective.
 A port fuel-injected engine that is equipped with long, tuned intake-manifold runners.
A port fuel-injected engine that is equipped with long, tuned intake-manifold runners.