Please identify the documented ROS elements and the supporting findings. How does the documented ROS provide greater information about the CC and the HPI?
HPI: 68-year-old male presents to the Emergency Department with a four-day history of loose stools. Patient states that over the past several days he has had at least six to 10 loose, watery stools per day. No hematochezia or melena. He denies any fever or abdominal pain. No chest pain, shortness of breath, or peripheral edema. Did see his primary care physician several days ago, who increased his metoprolol to 100 mg daily.
PMH:
1. Coronary artery disease, status post CABG 2002
2. Sternal osteomyelitis, status post CABG
3. Gout
4. Chronic renal insufficiency, baseline creatinine 2.0
5. Ischemic cardiomyopathy, last echocardiogram 5/21/2012, EF 32
6. Peripheral neuropathy
7. Diabetes Mellitus, type II (noninsulin dependent)
8. Hypertension
9. Appendiceal abscess, hospitalized 3/2010 to 4/2010, treated by conservative medical management only
10. Mild COPD
ROS: As per HPI.
Medications:
1. Metoprolol ER 100 mg by mouth daily (dose increased three days ago)
2. Amitriptiline 25 mg by mouth at night
3. Plavix 75 mg by mouth daily
4. Aspirin 81 mg by mouth daily
5. Lisinopril 20 mg by mouth daily
6. Spirinolactone 25 mg by mouth daily
7. Lasix 40 mg by mouth daily
8. Colchicine 0.6 mg by mouth daily
9. Simvistatin 20 mg by mouth every night
10. Glipizide 10 mg by mouth daily
What will be an ideal response?
Question 2
The documented PFSH is Pertinent.
29-year-old woman returns to clinic with severe cough. Over the past five days, cough has become more persistent. Throat burns constantly during day. No identified postnasal drip, although patient rates throat pain at 8/10 all the time. Both cough and pain are much worse after eating evening meal. Identifies pain along the length of throat, a burning in her chest, and reports that her mouth tastes sour along with the presence of excessive saliva in her mouth. Throat lozenges exacerbate the pain but alleviate the bitter taste in her mouth. Ice chips provide temporary relief for pain. Patient feels very anxious about pain, reporting heart palpitations and anxiety: father diagnosed with stage II squamous cell esophageal carcinoma 14 months ago. Patient engaged in smoking cessation program nine months ago after a 12-year smoking habit. In addition to HPI, patient reports loss of appetite. No report of nausea, fever chills, diarrhea, swollen joints, unusual muscle aches, headache, double vision, painful urination, or shortness of breath. No identified skin rash. History of peptic ulcer at age 14, responded well to OTC treatment with no recurrence. Occasional problem with heartburn, but patient admits she has not kept track of her own health due to schoolwork, job and father's health problems. Bronchitis complicated by pleurisy last year, responded well to ABX treatment. No history of asthma. No known drug allergies. Patient is a second year law student at Collegetown Law. Alcohol: two to four beers a week average.
Indicate whether this statement is true or false.

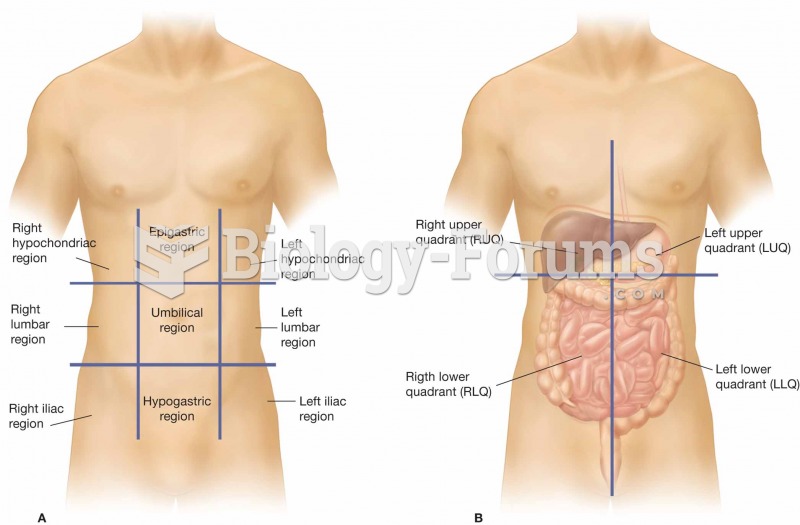 (A) The nine regions of the abdominopelvic cavity. (B) The four regions of the abdomen, which are re
(A) The nine regions of the abdominopelvic cavity. (B) The four regions of the abdomen, which are re
 Infanticide in nonhuman primates has been best-documented in Hanuman langurs.
Infanticide in nonhuman primates has been best-documented in Hanuman langurs.
 B. F. Skinner documented how operant conditioning changes behavior.
B. F. Skinner documented how operant conditioning changes behavior.
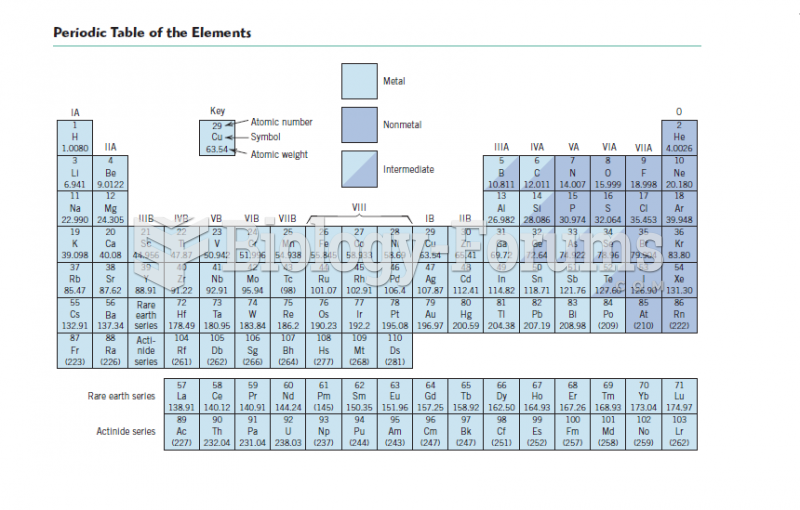 Periodic Table of the Elements
Periodic Table of the Elements
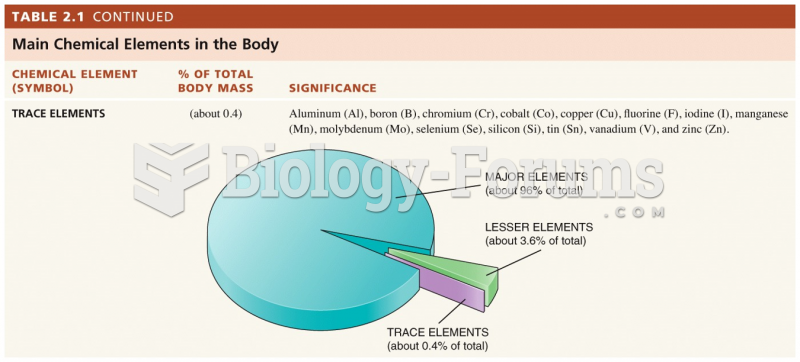 Trace Elements of the Human Body
Trace Elements of the Human Body
 The elements with these exceptions are
The elements with these exceptions are