Answer to Question 1
C
The patient's behavior is consistent with a panic level of anxiety. Calm, brief, directive verbal instructions can help such patients gain control of overwhelming feelings and impulses. Patients experiencing panic-level anxiety are unable to focus and integrate new information into memory, making teaching likely to be ineffective until their anxiety is reduced. Antianxiety medications and seclusion would be a back-up intervention if verbal interventions fail. However, although providing an opportunity for the patient to participate in decisions about his care is usually desirable, asking the patient to choose the route of medication to be used at a time when understanding and decision making are impaired is not therapeutic. Seclusion could be interpreted as punishment or perceived as a threat, and in turn heighten his fear and panic; it should be reserved for situations when all other options have failed or no other intervention can provide acute safety needs.
Answer to Question 2
A
The DSM-IV-TR description of depersonalization disorder states that it involves a persistent or recurrent experience of feeling detached from and outside one's mental processes or body. Although reality testing is intact, the experience causes significant impairment in social or occupational functioning and distress to the individual. Body dysmorphic disorder involves preoccupation with a body part the individual believes to be distorted. Dissociative amnesia involves memory loss. Malingering is a conscious effort to deceive others, often for financial gain, by pretending to have physical symptoms.

 Choose the telephone unit that offers the features needed in your office.
Choose the telephone unit that offers the features needed in your office.
 Douglas Gordon, 24 Hour Psycho.
Douglas Gordon, 24 Hour Psycho.
 The medical assistant escorts the patient into the examination room.
The medical assistant escorts the patient into the examination room.
 Calipers are used to measure the body fat on the triceps of a patient.
Calipers are used to measure the body fat on the triceps of a patient.
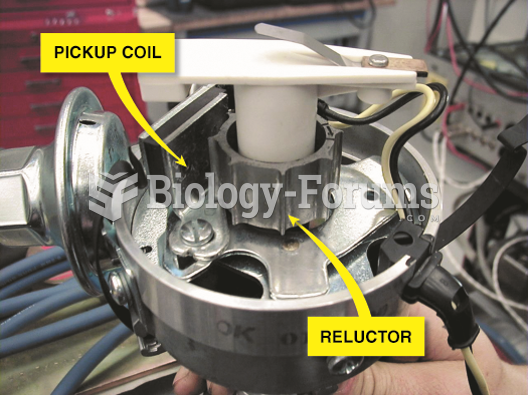 A Chrysler electronic ignition distributor. This unit is equipped with a vacuum advance mechanism ...
A Chrysler electronic ignition distributor. This unit is equipped with a vacuum advance mechanism ...
 Jaundice seen in the eyes and the skin of a patient with hepatitis A.
Jaundice seen in the eyes and the skin of a patient with hepatitis A.