Answer to Question 1
Correct Answer: 1,2
Rationale 1: Consistent high amounts of corticosteroid medications provide continuous negative feedback to the hypothalamus and pituitary, shutting down the secretion of ACTH.
Rationale 2: Without stimulation by ACTH, the adrenal cortex shrinks and stops secreting endogenous corticosteroids.
Rationale 3: Acute adrenocortical insufficiency is not caused by rebound ACTH secretion.
Rationale 4: Acute adrenocortical insufficiency is not caused by excessive secretion of ACTH.
Rationale 5: Mineralocorticoids do not cause acute adrenal insufficiency.
Global Rationale: Consistent high amounts of corticosteroid medications provide continuous negative feedback to the hypothalamus and pituitary, shutting down the secretion of ACTH. Without stimulation by ACTH, the adrenal cortex shrinks and stops secreting endogenous corticosteroids. Acute adrenocortical insufficiency is not caused by rebound ACTH secretion, by excessive secretion of ACTH, or by mineralocorticoid levels.
Answer to Question 2
Correct Answer: 1,2
Rationale 1: Open-angle glaucoma is a frequent adverse effect of long-term corticosteroid therapy.
Rationale 2: Cataracts are a frequent adverse effect of long-term corticosteroid therapy.
Rationale 3: Detached retina is not an adverse effect of long-term corticosteroid therapy.
Rationale 4: Retinopathy is not an adverse effect of long-term corticosteroid therapy, although it might occur as an effect of uncontrolled blood glucose levels, as seen in diabetes mellitus.
Rationale 5: Macular degeneration is not an adverse effect of long-term corticosteroid therapy.
Global Rationale: Open-angle glaucoma and cataracts are frequent adverse effects of long-term corticosteroid therapy. Retinopathy is not an adverse effect of long-term corticosteroid therapy, although it might occur as an effect of uncontrolled blood glucose levels, as seen in diabetes mellitus. Macular degeneration and detached retina are not adverse effects of long-term corticosteroid therapy.

 A nurse shows empathy to a client.
A nurse shows empathy to a client.
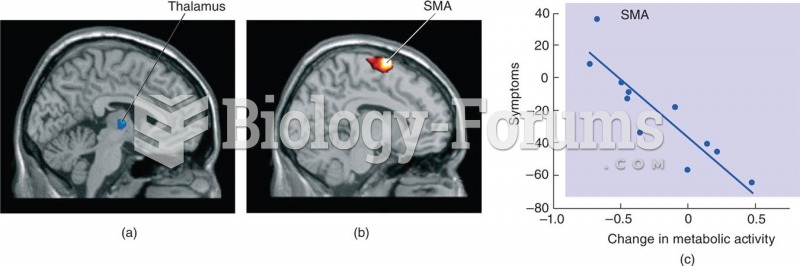 Gene Therapy of Parkinson’s Disease
Gene Therapy of Parkinson’s Disease
 Seven black members of Congress in 1871 are from left to right: Senator Hiram Revels (R-MS) and Repr
Seven black members of Congress in 1871 are from left to right: Senator Hiram Revels (R-MS) and Repr
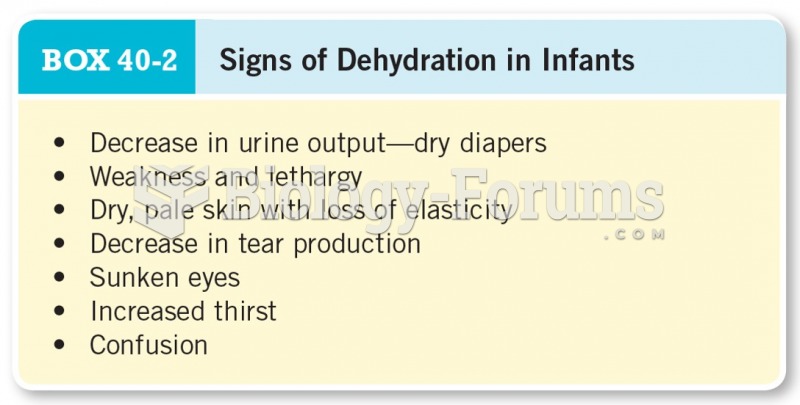 Signs of Dehydration in Infants
Signs of Dehydration in Infants
 Towels have many uses during a massage therapy session.
Towels have many uses during a massage therapy session.
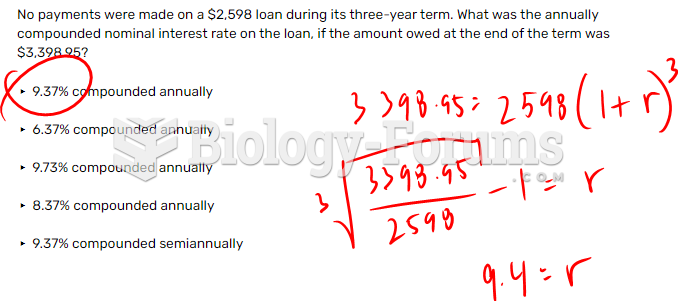 No payments were made on a $2,598 loan during its three-year term. What was the annually ...
No payments were made on a $2,598 loan during its three-year term. What was the annually ...