Answer to Question 1
Correct Answer: 1
During the health history for a pediatric client, it is appropriate for the nurse to ask the client which grade they are currently in. Monitoring the client's vital signs and assessing the client's cardiovascular system would be completed in the physical examination, not the health history portion of the assessment. Documenting immunizations administered during the current visit would occur after the nurse administers them prior to the close of the assessment, not during the health history.
Answer to Question 2
Correct Answer: 3, 1, 4, 2
S refers to subjective data that are provided by the client regarding the symptoms that the client is experiencing. O refers to objective data. The nurse documents information about the signs that the client is exhibiting. A refers to assessment. The nurse draws conclusions regarding the subjective and objective data that the nurse has collected about the client. P refers to planning. Planning indicates that interventions that the nurse can use to help resolve the client's problems or address the client's needs.

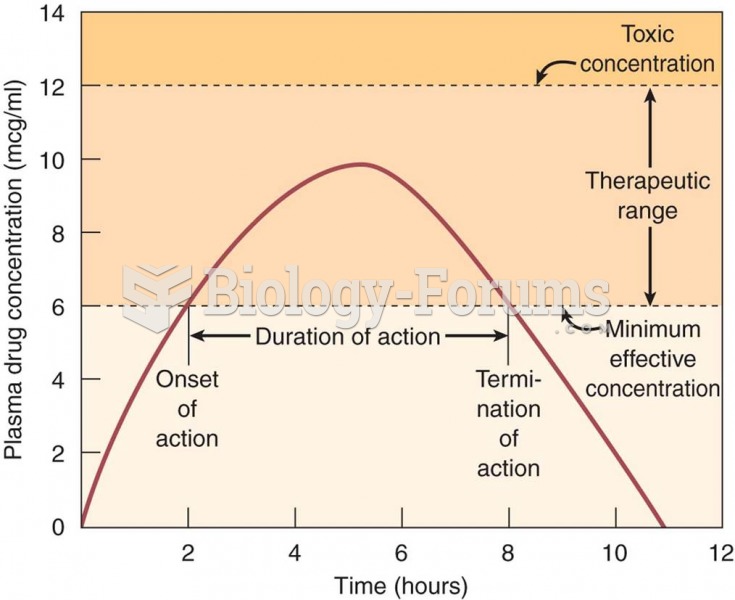 Single-dose drug administration: pharmacokinetic values for this drug are as follows: onset of actio
Single-dose drug administration: pharmacokinetic values for this drug are as follows: onset of actio
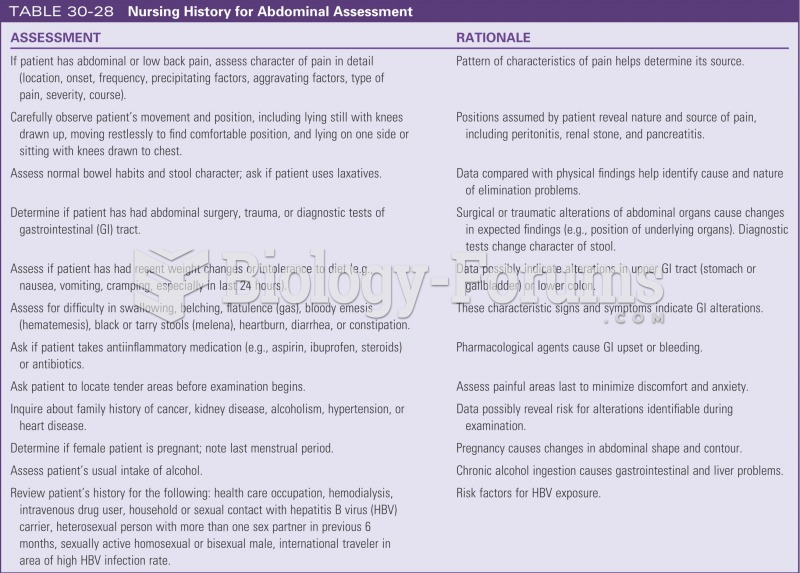 Nursing history for abdominal assessment
Nursing history for abdominal assessment
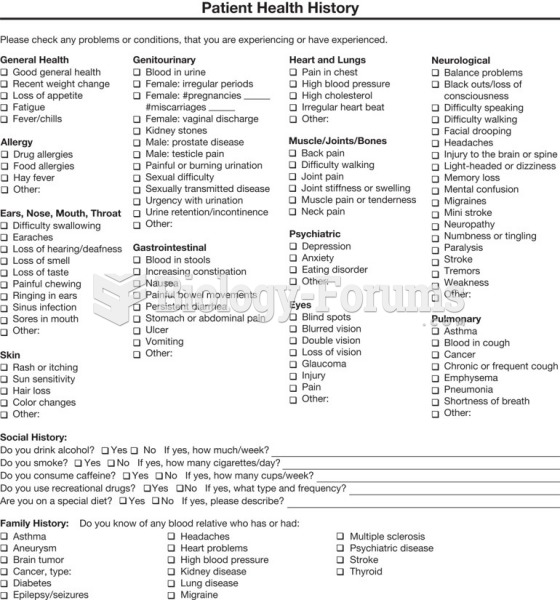 Patient health history form Cont.
Patient health history form Cont.
 Nurse using a stethoscope
Nurse using a stethoscope
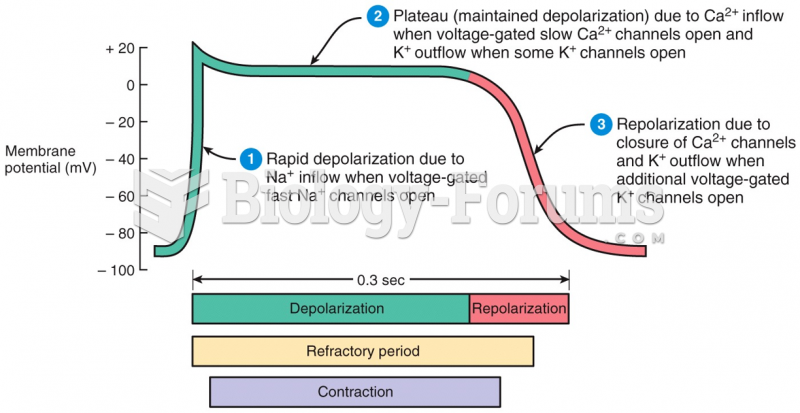 Action Potential in a Ventricular Fiber
Action Potential in a Ventricular Fiber
 Tissue-specific enhancer action
Tissue-specific enhancer action