EMERGENCY ROOM REPORT
HISTORY OF PRESENT ILLNESS: This 18-year-old white male presents to the emergency room by private vehicle for evaluation of abrasion injuries. The patient states that last night he was riding a motorcycle when he slipped on some gravel. He was not wearing a helmet but denies any loss of consciousness or neck injury. His only complaint is of the right forearm and right knee area being deep abrasions. He, in addition, suffered minor abrasions to his right cheek and to his chest/abdomen area. He denies any shortness of breath. No numbness, tingling, weakness to an arm or a leg. Tetanus is up to date being two years ago.
ALLERGIES: NONE KNOWN.
CURRENT MIDDICATIONS: None.
PAST MEDICAL HISTORY: Unremarkable.
PHYSICAL EXAM:
Blood pressure 140/64, temperature 99.6 F, pulse 100, respirations 24. In general appears a well-developed alert male who appears in minimal discomfort.
HEENT: Shows mild amount of abrasions to the right cheekbone area. There is no evidence of bony tenderness in this area. Funduscopic exam and pupil exam are normal. Ears normal.
NECK: Soft, supple. No thyromegaly or lymphadenopathy. Cervical spine is nontender to firm palpation and range of motion. Skull was nontender either.
NEUROLOGIC: Normal for light touch sensation and muscle strength testing.
EXTREMITIES: Exam of the right forearm area shows deep abrasions about the forearm itself, not about the elbow. Elbow range of motion was quite good. There is no evidence of elbow effusion. No evidence of bony tenderness to the forearm. Examination of the right knee revealed deep abrasions anteriorly, some gravel foreign body present. None of these abrasions appears to be full skin thickness in nature. Knee itself showed no evidence of effusion. The patient was tender only about the abrasions. Knee range of motion and full extension to 90 degrees of flexion and ligamentous testing was normal.
DISCUSSION: I told the patient I would recommend a knee x-ray given the amount of trauma that was sustained to the skin of the area and the decreased range of motion. The patient refused a knee x-ray though. For treatment of his abrasions, I wanted to send him to physical therapy for whirlpool treatment and debridement as needed. The patient refused to do this, citing financial concerns as a reason why. Therefore, I had our emergency nurse thoroughly debride all of these wounds as best as possible. The patient was instructed to follow up with a private physician as soon as possible. I am still giving him a note for physical therapy that he may follow up with them if he so chooses. The patient is to return for any sign of infection or other problems.
IMPRESSION: Deep abrasions to right forearm and right knee area.
PLAN: General wound care instructions given. He is told to return to the emergency department if any problems or sign of infection or other complaints.
ICD-9-CM diagnosis code(s): ___________________ __
ICD-10-CM diagnosis code(s): ___________________ __
CPT code(s) with modifier, if applicable: ___________________ __
APC: ___________________ __
What will be an ideal response?
Question 2
The immunization record is typically found in what setting?
A. Acute inpatient
B. Physician office
C. Emergency department
D. Same-day surgery

 Decorative white silk crosses are an ingenious tactic used by orb-weaving spiders to protect their w
Decorative white silk crosses are an ingenious tactic used by orb-weaving spiders to protect their w
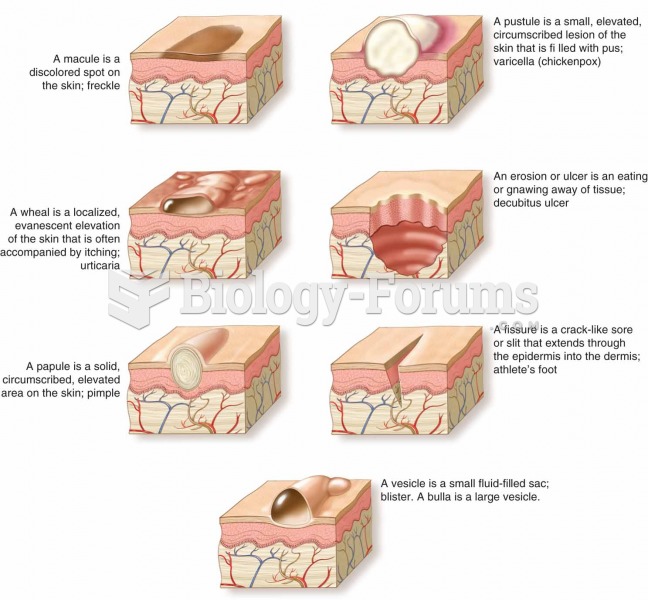 Skin signs are objective evidence of an illness or disorder. They can be seen, measured, or felt.
Skin signs are objective evidence of an illness or disorder. They can be seen, measured, or felt.
 Defibrillator. Defibrillators are devices that supply a voltage charge to the heart in the hope of r
Defibrillator. Defibrillators are devices that supply a voltage charge to the heart in the hope of r
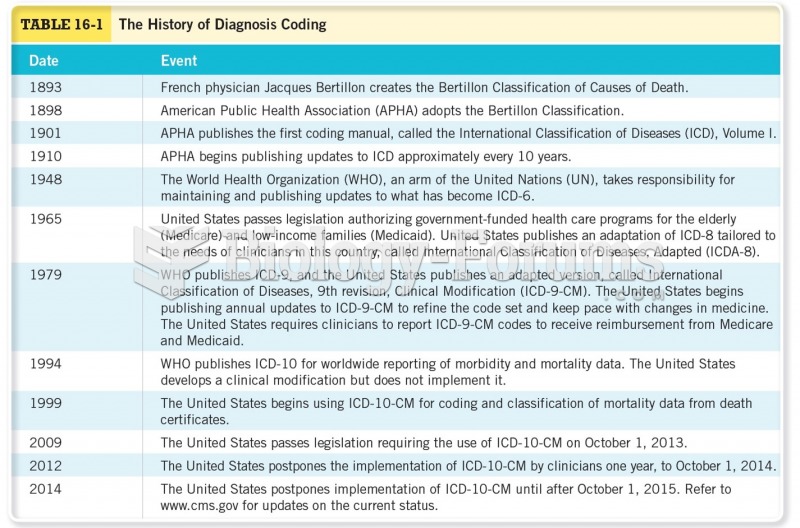 The History of Diagnosis Coding
The History of Diagnosis Coding
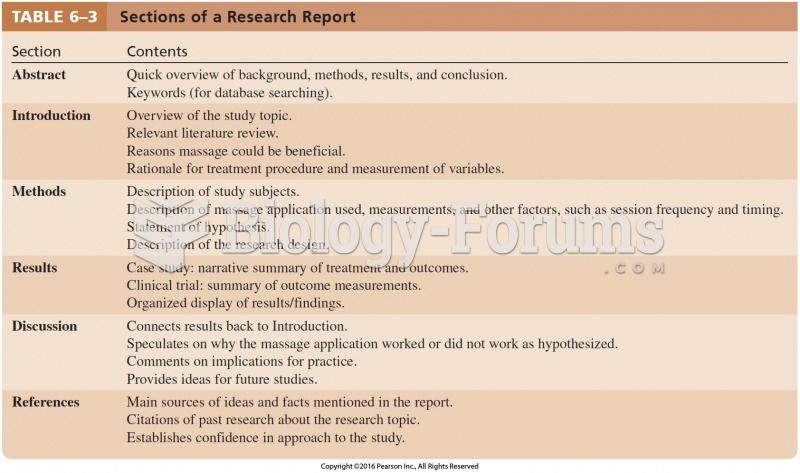 Sections of a Research Report
Sections of a Research Report
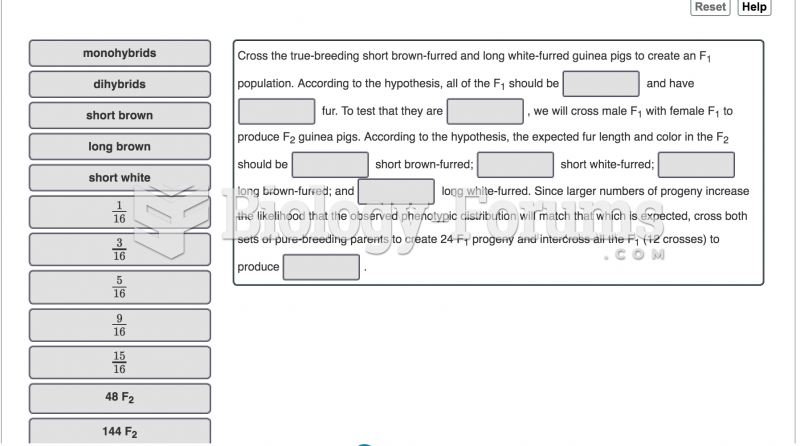 You have four guinea pigs for a genetic study. One male and one female are from a strain that ...
You have four guinea pigs for a genetic study. One male and one female are from a strain that ...