A patient admitted to the hospital has been using phenylephrine nasal spray (Neo-Synephrine), 2 sprays every 4 hours, for a week.
The patient complains that the medication is not working, because the nasal congestion has increased. What will the nurse do?
a. Request an order for an oral decongestant to replace the intranasal phenylephrine.
b. Request an order for an intranasal glucocorticoid to be used while the phenylephrine is withdrawn.
c. Tell the patient to increase the dose of phenylephrine to 4 sprays every 4 hours.
d. Tell the patient to stop using the phenylephrine and begin using an intranasal antihistamine.
Question 2
A patient with allergic rhinitis is taking a compound product of loratadine/pseudoephedrine (Claritin-D) every 12 hours. The patient complains of insomnia. The nurse notes that the patient is restless and anxious.
The patient's heart rate is 90 beats per minute, and the blood pressure is 130/85 mm Hg. The nurse will contact the provider to:
a. discuss using an intranasal glucocorticoid and loratadine (Claritin).
b. report acute toxicity caused by pseudoephedrine.
c. suggest using an agent with a sympathomimetic drug only.
d. suggest using a topical decongestant to minimize systemic symptoms.

 Measuring Patient Height
Measuring Patient Height
 Down Syndrome Nasal bridge
Down Syndrome Nasal bridge
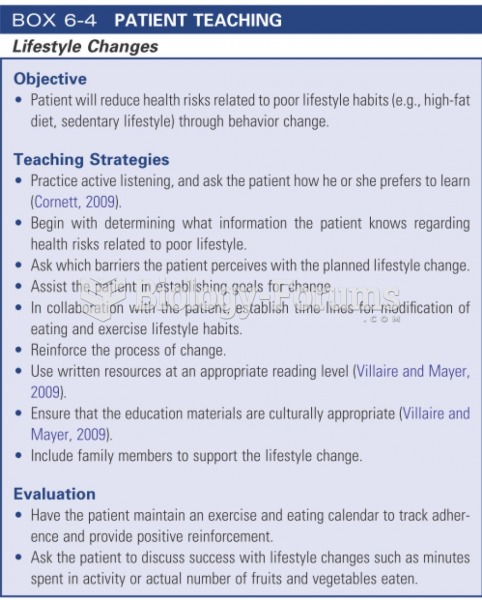 Patient Teaching
Patient Teaching
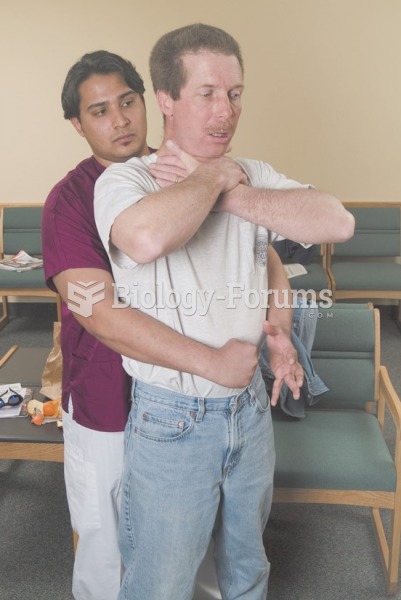 Abdominal thrusts are delivered with a firm thrust into the patient’s abdomen with an upward ...
Abdominal thrusts are delivered with a firm thrust into the patient’s abdomen with an upward ...
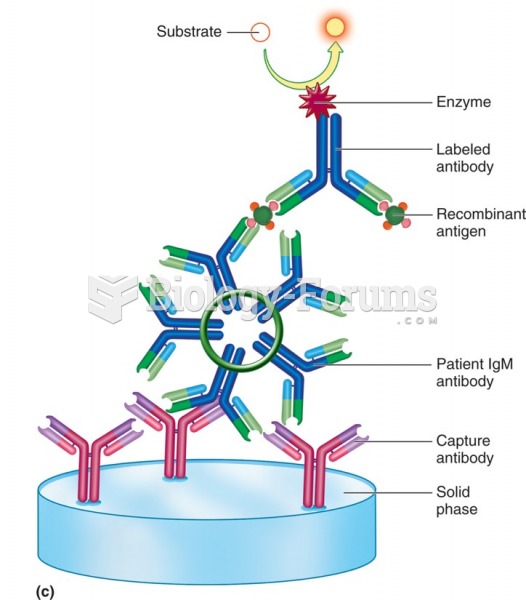 Sandwich or capture enzyme immunoassay for patient IgM (double capture: IgM capture, Ag capture).
Sandwich or capture enzyme immunoassay for patient IgM (double capture: IgM capture, Ag capture).
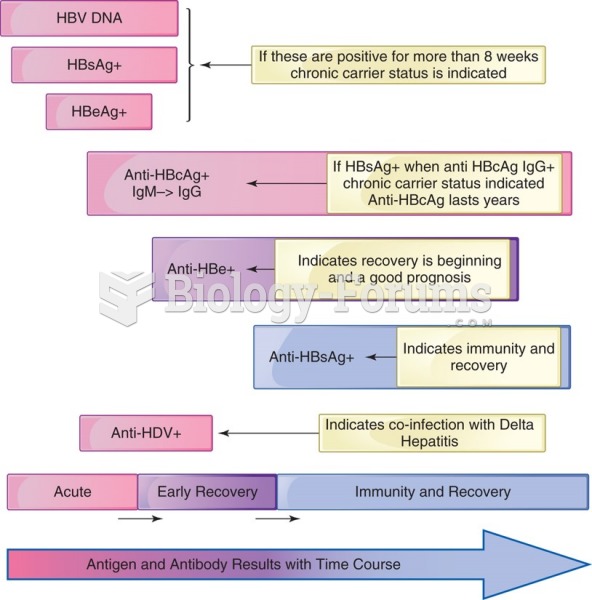 Hepatitis B antigens and antibody in an acutely infected patient with recovery. Note the indicators ...
Hepatitis B antigens and antibody in an acutely infected patient with recovery. Note the indicators ...