Answer to Question 1
DSM-5 requires that the erotic preoccupation must have lasted at least six months before the person would meet diagnostic criteria for a paraphilic disorder. Furthermore, the diagnosis of paraphilic disorder is made only if the person's paraphilic urges lead to clinically significant distress or impairment. The person would be considered to be impaired if the urges have become compulsory, if they produce sexual dysfunction, if they require the participation of nonconsenting persons, if they lead to legal problems, or if they interfere with social relationships.
Answer to Question 2
Although DSM-5 includes unusually low sexual desire as a sexual dysfunction, it does not mention unusually high sexual desire. A proposal was submitted, and ultimately rejected, to include hypersexual disorder. Symptoms associated with this disorder would include seeking new sexual encounters out of boredom with old ones, frequent use of pornography, and legal problems resulting from sexual behaviors. Additional features include obsessive thoughts about sexual encounters, guilt resulting from problematic sexual behavior, and rationalization for continued reckless sexual behavior. There are several good reasons to be skeptical of this concept. Perhaps most important is the heterogeneous nature of excessive or uncontrolled sexual behavior. Failure to control sexual impulses can be associated with several other disorders, including paraphilic disorders, impulse control disorders, and bipolar disorder. Many people who admit to compulsive sexual behavior also suffer from major depression, anxiety disorders, and substance use disorders. The concept obviously includes a diverse set of behavioral problems. It also suffers from conceptual problems that have been raised with regard to impulse control disorders and behavioral addictions. For all of these reasons, the proposal for recognizing hypersexual disorder as a new diagnosis in DSM-5 was rejected.

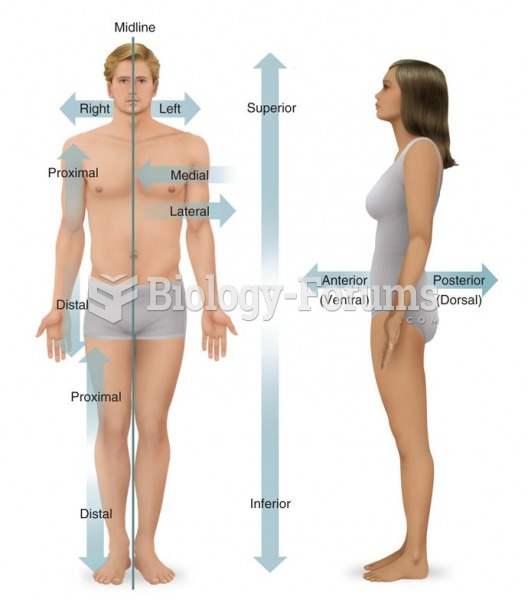 Relative Positional Terms
Relative Positional Terms
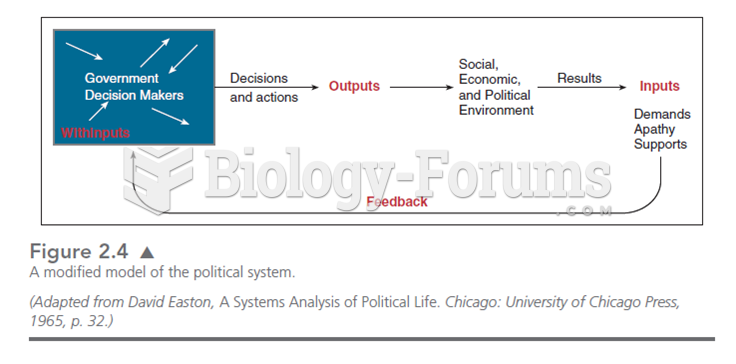 This modified model of Easton’s systems theory puts government decision makers as the source of pol
This modified model of Easton’s systems theory puts government decision makers as the source of pol
 The relative influence of heredity and the environment in human behavior has fascinated and plagued ...
The relative influence of heredity and the environment in human behavior has fascinated and plagued ...
 Social scientists have not done well at devising theories to explain lovely romantic moments
Social scientists have not done well at devising theories to explain lovely romantic moments
 Explain how it can be desirable from an intertemporal perspective for a country run a current ...
Explain how it can be desirable from an intertemporal perspective for a country run a current ...
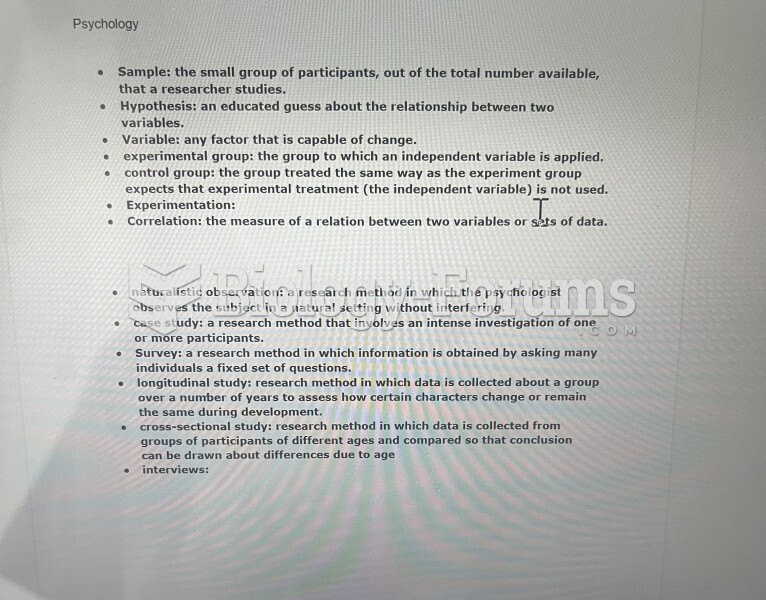 expiremntal psychology and its terms
expiremntal psychology and its terms