Answer to Question 1
In non-Hodgkin disease, there is a malignant transformation of either B or T lymphocytes. The key feature of Hodgkin disease is the presence of the Reed-Sternberg cella cell not found in non-Hodgkin disease.
Non-Hodgkin disease is multicentric in nature and often presents with painless, generalized lymphadenopathy with nonnodal concentration, or with several nodes involved. Hodgkin disease begins as a single enlarged node or within a local group. Typically HL begins in nodes above the diaphragm in the younger population. In elderly individuals, it may initially present in nodes below the diaphragm.
Rituximab is a pharmaceutic monoclonal antibody (MOA). It acts by recognizing and binding to the CD20 antigen found on the majority of B-cell lymphomas. After binding, the toxic effect of the MOA destroys the malignant cell.
The parenchyma consists of a cortex, paracortex, and medulla. In the cortex, B cells are found in the primary follicles and secondary follicles. Within the secondary follicles are immunologically active germinal centers. B cells also surround the germinal centers in regions called mantle zones. T cells are also present in lymph nodes and are concentrated in the in the deeper region of the cortex known as the paracortex.
Max's follicular lymphoma involved the centroblasts and centrocytes in the germinal centers of the lymph nodes.
Answer to Question 2
being overweight, smoking, family history of heart disease, and low serum HDL and high serum LDL levels.
An excessive caloric intake lowers HDL levels. Elevated serum cholesterol levels are affected not only by dietary intake of cholesterol but also by a diet high in saturated fats. Hypercholesterolemi a results in increased VLDL and LDL levels in the blood. Trans fat is emerging as the most potent atherogenic lipid, and limiting dietary levels of this fat is important in managing the at-risk patient.
Smoking is thought to contribute to oxidative processes in the lumen of vessels and consequent damage to the endothelium. Furthermore, smoking is thought to magnify endothelial dysfunction when it is already present in predisposed individuals. Finally, smoking decreases circulating levels of HDL. Unlike smoking, exercise increases serum HDL levels. High levels of HDL are inversely related to the development of atherosclerosis and coronary artery disease. These lipoproteins clear cholesterol from atheromatous plaques and move them to the liver for excretion from the body. It is believed they also inhibit the cellular uptake of LDL.
Monocytes migrate to the subendothelial space in blood vessels and become macrophages. Once activated, macrophages release free radicals to oxidize LDL. Oxidized LDL subsequently destroys endothelial tissue. Macrophages also ingest oxidized LDL and form foam cells, a feature common to all atherosclerotic changes. Finally, macrophages promote the proliferation of smooth muscle cells and the deposition of the extracellular matrix at the lesion site.
Elevated levels of hs-CRP (a protein involved in the acute-phase inflammatory response) indicate systemic inflammation. It is now considered a major risk factor marker for cardiovascular disease.

 Older adults working
Older adults working
 This 19-year-old in Wisconsin was given a reduced jail sentence for holding this sign in front of ...
This 19-year-old in Wisconsin was given a reduced jail sentence for holding this sign in front of ...
 The remarkably complete skull of a 3-year-old Australopithecus girl; the fossil is 3.3 million ...
The remarkably complete skull of a 3-year-old Australopithecus girl; the fossil is 3.3 million ...
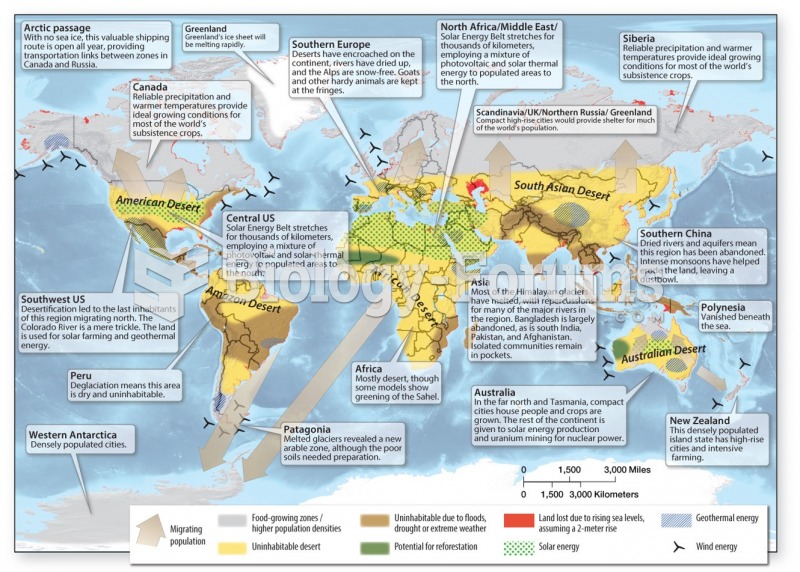 Water shortages, reduced agricultural capacity & coastal inundation are common themes
Water shortages, reduced agricultural capacity & coastal inundation are common themes
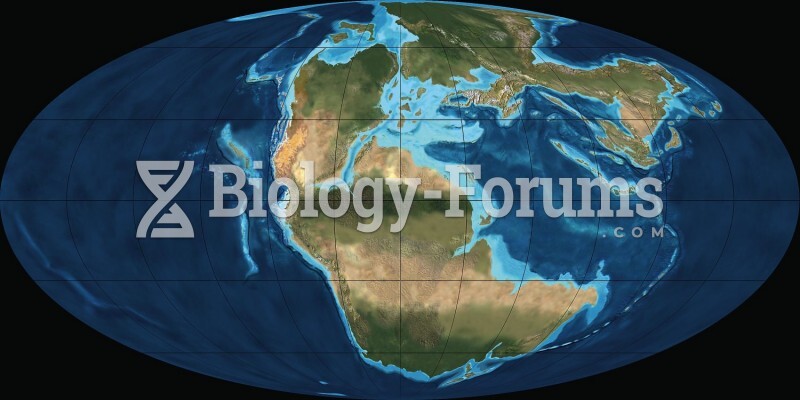 Earth 200 Million Years Ago
Earth 200 Million Years Ago