Answer to Question 1
The typical signs and symptoms of a fracture include pain, swelling, and loss of function. If long bones are involved, the deformity results from the angulation, rotation, or shortening of the involved bone. Typically, abnormal mobility is also evident at the site of injury.
A decrease in the feeling of pain shortly after the injury is termed local shock. It involves a temporary interruption of neural function at the fracture site so that both sensory and motor activity is lost.
A hematoma forms from the blood that escapes from the torn vessels of the injured periosteum and surrounding soft tissues. It encircles and invades the fracture site to deliver clotting factors so that a fibrin network can be laid down. This network forms a foundation for fibroblast activity and the migration of new capillary buds. The hematoma also contains activated inflammatory cells and platelets. The growth factors released from these cells stimulate the proliferation of osteoclasts and osteoblasts for the deposition and remodeling of new bone.
The immobilization necessary for fracture healing also promotes joint stiffness through tendon shortening and disuse atrophy of the muscles. The cast is therefore removed as soon as possible to minimize the negative effects of immobilization. Exercises introduced early in the healing process help to maintain tissue integrity and are done bilaterally. A thorough rehabilitation program would include a full range of motion exercises for his unaffected arm and isometric (or muscle-tensing) exercises for his affected arm.
Answer to Question 2
Mandy is likely demonstrating the effects of the female athletic triad. Disordered eating and intensive exercise in some athletes reduce fat stores and the fat-to-muscle ratio. The result is a decrease in estrogen production by the ovaries with amenorrhea. The reduction in circulating estrogen, coupled with an insufficient intake of vitamin D and calcium, accelerates bone resorption and the formation of osteoporosis.
Estrogen deficiency contributes to the development of osteoporosis in a number of ways. Lowered levels of estrogen encourage an increase in cytokine production that stimulates the proliferation of osteoclast precursors. Furthermore, when estrogen is low, the differentiation of osteoclasts becomes unregulated; osteoclast precursors are more responsive to the RANK ligand, and osteoclastic proliferation occurs. The result is a condition of bone resorption that occurs at a rate that cannot be matched by a compensatory increase in osteoblastic activity.
Osteoporosis is a disease characterized by a decline in bone mass. Osteoporotic bone is porous and brittle with a decreased amount of trabeculae and cortical volume. Osteomalacia, in contrast, is a disease characterized by the undermineralization of bone. Bone tissue exhibiting osteomalacia is soft and weak due to the lack of mineralization. Total bone mass, however, is unchanged.

 The bobcat population has seen declines in the American Midwest, but is generally stable and healthy
The bobcat population has seen declines in the American Midwest, but is generally stable and healthy
 Trans-Alaska Pipeline System (TAPS) Crosses the Active Strike-Slip Denali Fault
Trans-Alaska Pipeline System (TAPS) Crosses the Active Strike-Slip Denali Fault
 The driver information display on a Chevrolet Impala with a 5.3 liter V-8 equipped with active fuel ...
The driver information display on a Chevrolet Impala with a 5.3 liter V-8 equipped with active fuel ...
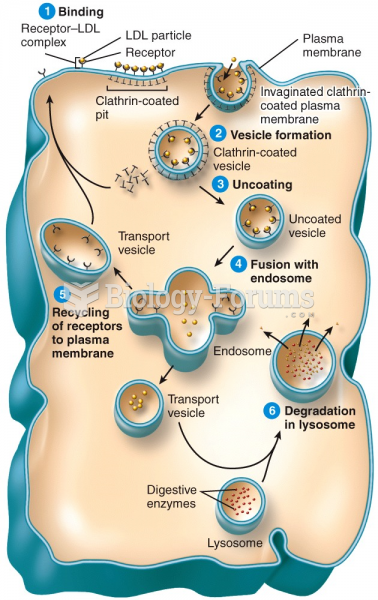 Active Transport in Vesicles: Receptor-mediated Endocytosis
Active Transport in Vesicles: Receptor-mediated Endocytosis
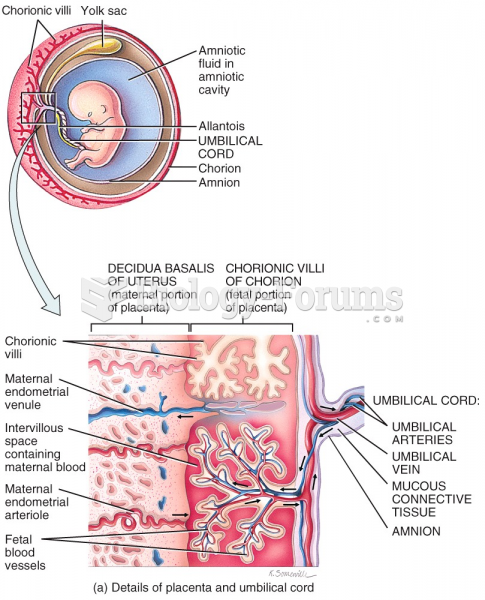 Embryonic Period - 12th week
Embryonic Period - 12th week
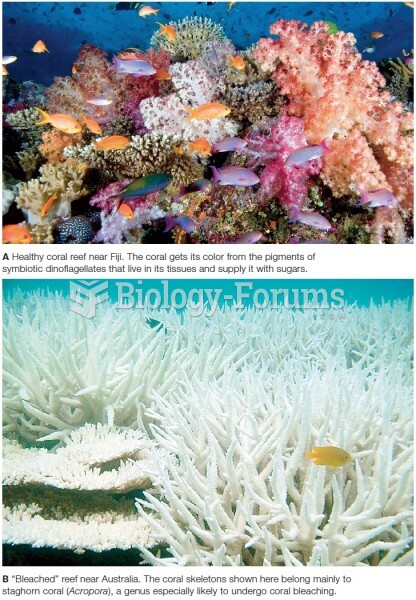 Healthy and damaged coral reefs.
Healthy and damaged coral reefs.