Answer to Question 1
3
Explanation:
1. RhoGAM is administered to prevent sensitization after exposure to Rh-positive blood.
2. An antibody screen (indirect Coombs test) is done to determine whether an Rh-negative woman is sensitized (has developed isoimmunity) to the Rh antigen.
3. Unlike the situation with Rh incompatibility, antepartum treatment of ABO incompatibility is not warranted because it does not cause severe anemia. As part of the initial assessment, however, the nurse should note whether the potential for an ABO incompatibility exists in order to alert healthcare providers to the need for carefully assessing the newborn for the development of hyperbilirubinemia.
4. Unlike the situation with Rh incompatibility, antepartum treatment of ABO incompatibility is not warranted because it does not cause severe anemia.
Answer to Question 2
2
Explanation:
1. In most cases, ABO incompatibility is limited to type O mothers with a type A or B fetus. The group B fetus of a group A mother and the group A fetus of a group B mother are only occasionally affected.
2. In most cases, ABO incompatibility is limited to type O mothers with a type A or B fetus. The group B fetus of a group A mother and the group A fetus of a group B mother are only occasionally affected.
3. The incompatibility occurs as a result of the maternal antibodies present in her serum and interaction between the antigen sites on the fetal red blood cells (RBCs).
4. Group O infants, because they have no antigenic sites on the red blood cells (RBCs), are never affected regardless of the mother's blood type.

 An adult male giraffe feeding high up on an acacia
An adult male giraffe feeding high up on an acacia
 Establishing a caring and trusting relationship helps the client come to terms with a terminal illne
Establishing a caring and trusting relationship helps the client come to terms with a terminal illne
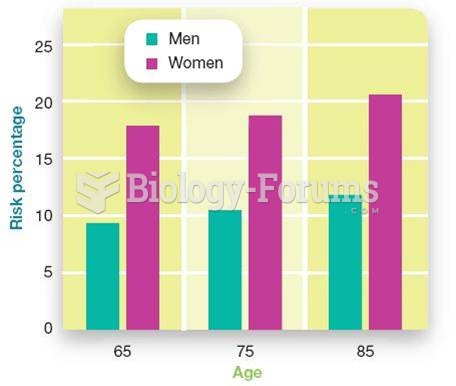 Alzheimer's Disease Risk
Alzheimer's Disease Risk
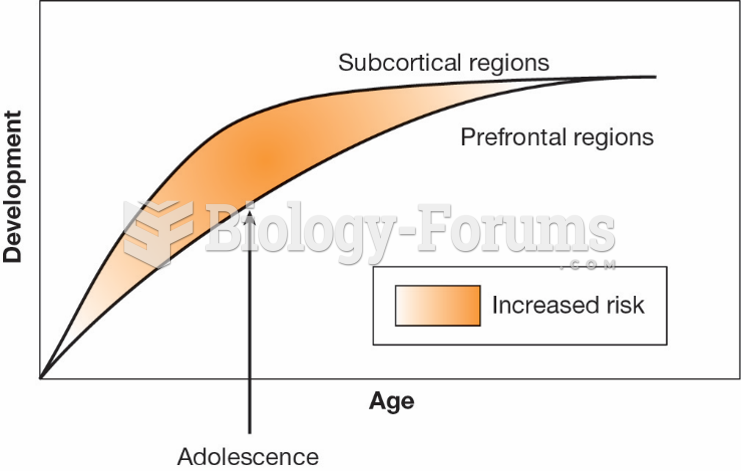 Dual Systems Model of Risk-Taking
Dual Systems Model of Risk-Taking
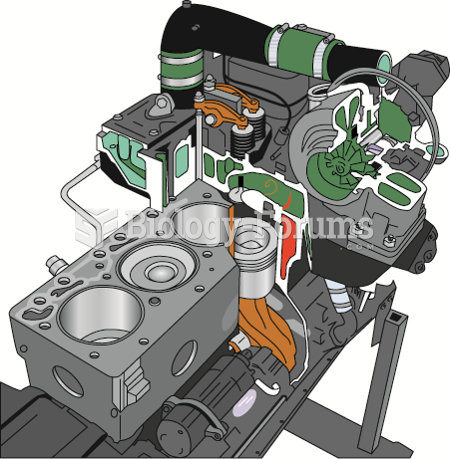 The common rail on a Cummins diesel engine. A high-pressure pump (up to 30,000 PSI) is used to ...
The common rail on a Cummins diesel engine. A high-pressure pump (up to 30,000 PSI) is used to ...
 Protein Needs Are Determined by Nitrogen Balance in Your Body
Protein Needs Are Determined by Nitrogen Balance in Your Body