Answer to Question 1
ANS: C
A. Incorrect response: See explanation C.
B. Incorrect response: See explanation C.
C. Correct response: Pressure-controlled ventilation (PCV) does not guarantee a volume, rather it controls inspiratory airway pressure. Volume is the dependent variable, and will change as lung mechanics or patient effort change. Sudden worsening of airway resistance with pressure targeted ventilation results in a loss of volume, but maximal airway pressures will not rise.
D. Incorrect response: See explanation C
Answer to Question 2
ANS: B
A. Incorrect response: Increasing the tidal volume when a patient is experiencing difficulty triggering a breath is inappropriate. The sensitivity setting may need to be adjusted, or the presence of auto-PEEP needs to be determined. If auto-PEEP is present, the following methods can be employed to reduce it: (1) increasing the inspiratory flow, (2) lengthening Te, (3) reducing the Vt, (4) reducing the respiratory rate, (5) using low resistance exhalation valves, (6) using a larger ETT, and (7) instituting applied PEEP.
B. Correct response: Increasing the Vt to 8 ml/kg may be appropriate when mechanically ventilating a patient for respiratory failure from airflow obstruction when the patient experiences severe patient-ventilator dyssynchrony or severe respiratory acidosis.
C. Incorrect response: Generally, the Fio2 is increased, or PEEP is added to elevate a patient's Pao2.
D. Incorrect response: Increasing the tidal volume when the inspiratory flow is inadequate is counterproductive. If the inspiratory flow is determined to be too low, the therapist should then increase that setting.

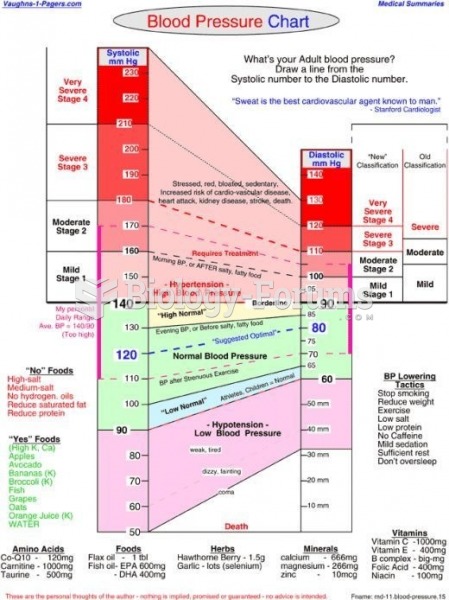 Blood Pressure Chart
Blood Pressure Chart
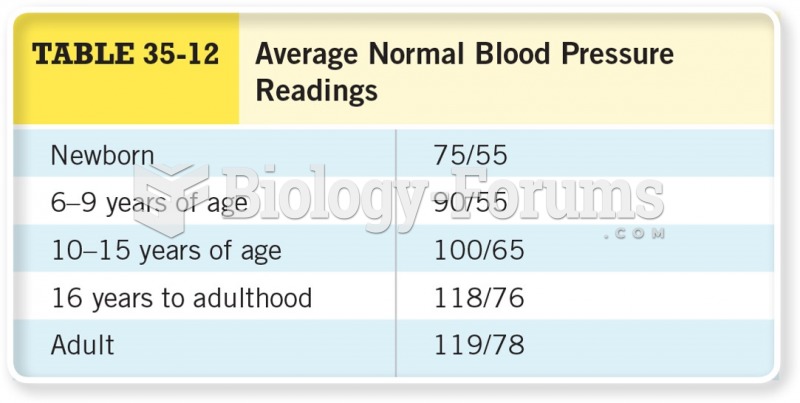 Average Normal Blood Pressure Readings
Average Normal Blood Pressure Readings
 Gingival enlargement in a patient taking nifedipine.
Gingival enlargement in a patient taking nifedipine.
 Gas pressure loss and venturi flowmeter
Gas pressure loss and venturi flowmeter