Answer to Question 1
ANS: D
If the endotracheal tube had slipped into the right mainstem bronchus, breath sounds would be heard on the right side and not on the left. The absence of breath sounds on the right side indi-cates that the endotracheal tube has not slipped into the right mainstem bronchus. No adventi-tious breath sounds are heard over the left lung, the patient has no history of bronchospasm, and no wheezing is heardthis essentially eliminates bronchospasm as the problem. The patient had been tolerating mechanical ventilation well for 5 days; therefore, the ET tube is not too small. The presence of auto-PEEP would cause hyperresonance to percussion bilaterally. The patient appar-ently has a pneumothorax on the right side, as evidenced by the absence of breath sounds and hyperresonance to percussion on that side.
Answer to Question 2
ANS: C
The lack of coordinated chest wall movement, the intercostal retractions, and the increased transairway pressure (seen at 1030) indicate bronchospasm. This can be confirmed by auscultat-ing the patient's chest. The patient should be suctioned before receiving the bronchodilator to remove any mucus. The sudden onset rules out an insidious increase in mucus. The ET tube is properly placed at the 20-cm mark and therefore does not require repositioning. This patient is not displaying any evidence of agitation, delirium, or anxiety; therefore, administration of haloperidol and midazolam is not appropriate in this situation. There is also no evidence of a need to change from volume to pressure control or to increase the set rate at this time.

 Pima Indian woman receiving an eye exam.
Pima Indian woman receiving an eye exam.
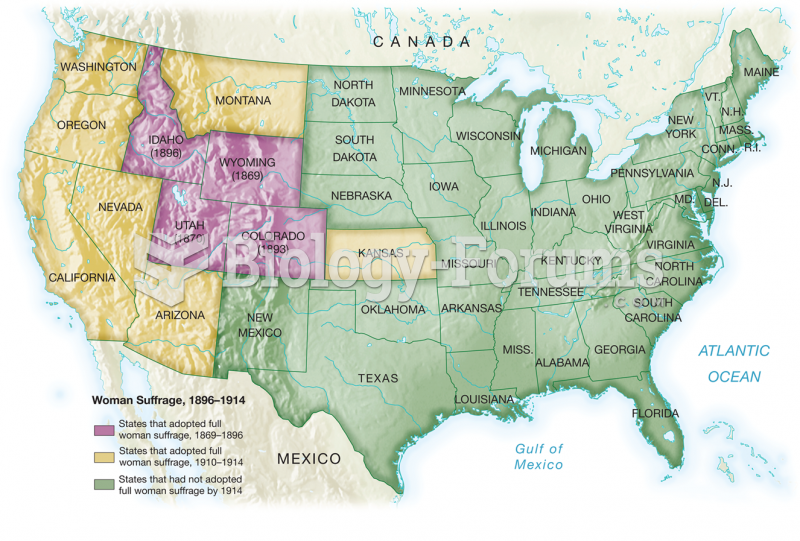 The Advance of Woman Suffrage
The Advance of Woman Suffrage
 Paul Colin, Figure of a Woman.
Paul Colin, Figure of a Woman.
 Pregnant woman taking precautions to prevent a toxoplasmosis infection by (a) having someone else ...
Pregnant woman taking precautions to prevent a toxoplasmosis infection by (a) having someone else ...
 The Beauty of a Woman
The Beauty of a Woman
 South American Indigenous Woman and Child
South American Indigenous Woman and Child