|
|
|

Did you know?
Methicillin-resistant Staphylococcus aureus or MRSA was discovered in 1961 in the United Kingdom. It if often referred to as a superbug. MRSA infections cause more deaths in the United States every year than AIDS.

 Nurse examining and measuring hematuria sample from client with a UTI
Nurse examining and measuring hematuria sample from client with a UTI
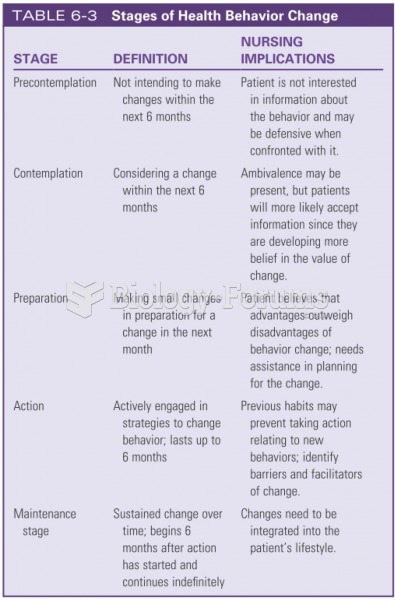 Stages of Health Behavior Change
Stages of Health Behavior Change
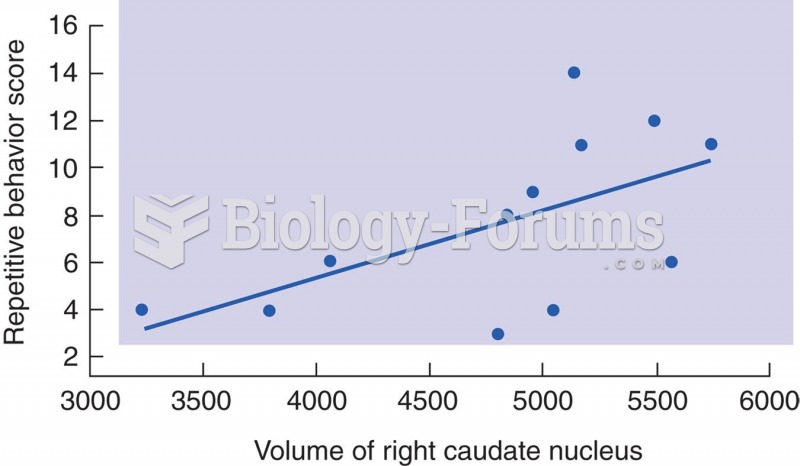 Caudate Nucleus and Stereotyped Behavior in Autism
Caudate Nucleus and Stereotyped Behavior in Autism
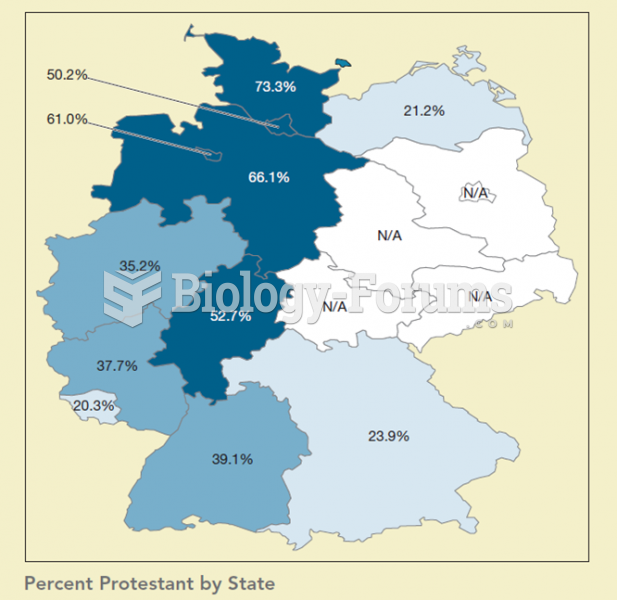 This map shows the percentage of Protestants by state in Germany. When compared to the previous map
This map shows the percentage of Protestants by state in Germany. When compared to the previous map
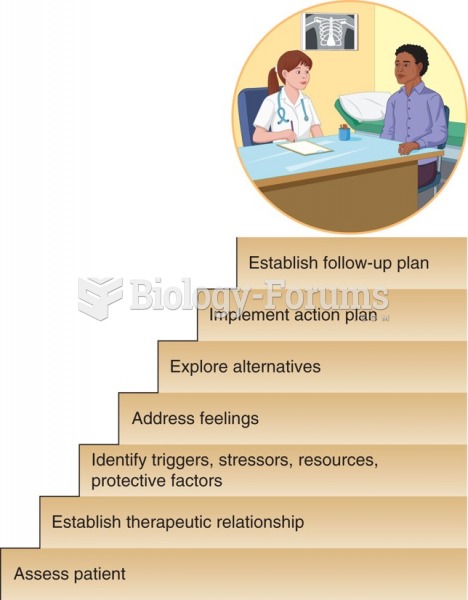 Roberts's Assessment, Crisis Intervention, and Trauma Treatment (ACT) model.
Roberts's Assessment, Crisis Intervention, and Trauma Treatment (ACT) model.
 Testing the Achilles tendon reflex with client in a supine position
Testing the Achilles tendon reflex with client in a supine position