This topic contains a solution. Click here to go to the answer
|
|
|

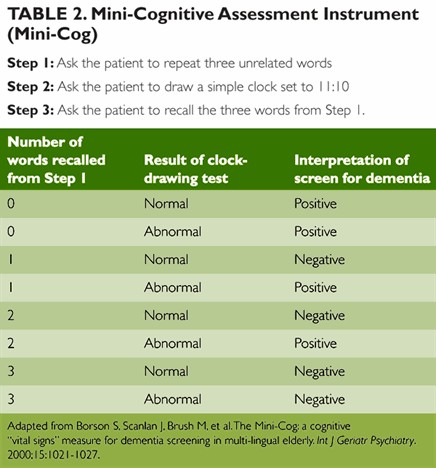 Health Assessment
Health Assessment
 An extended care facility.
An extended care facility.
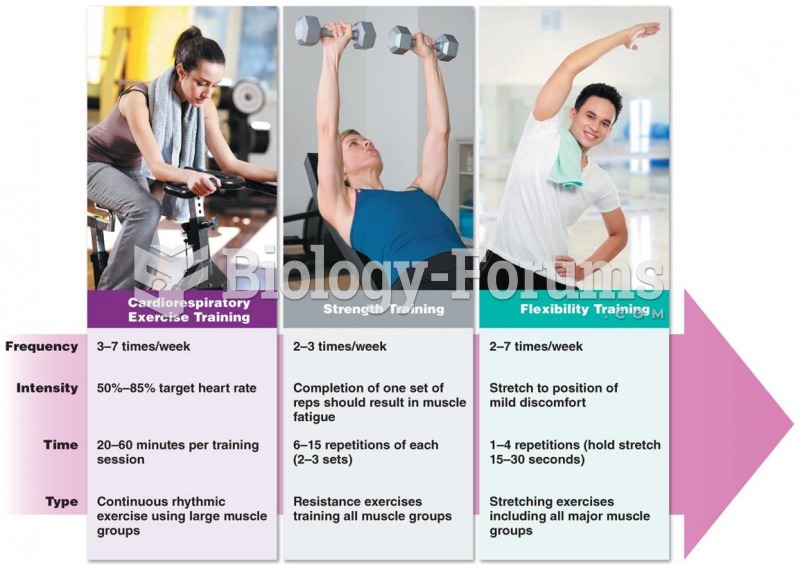 Applying the FITT Principle to Each Exercise Component of Health-Related Physical Fitness
Applying the FITT Principle to Each Exercise Component of Health-Related Physical Fitness
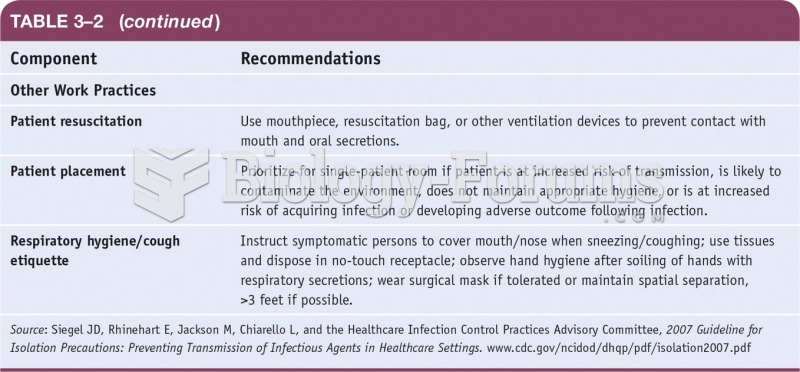 Standard Precautions for the Care of all Patients in All Health Care Settings
Standard Precautions for the Care of all Patients in All Health Care Settings
 The client is positioned for the examination
The client is positioned for the examination
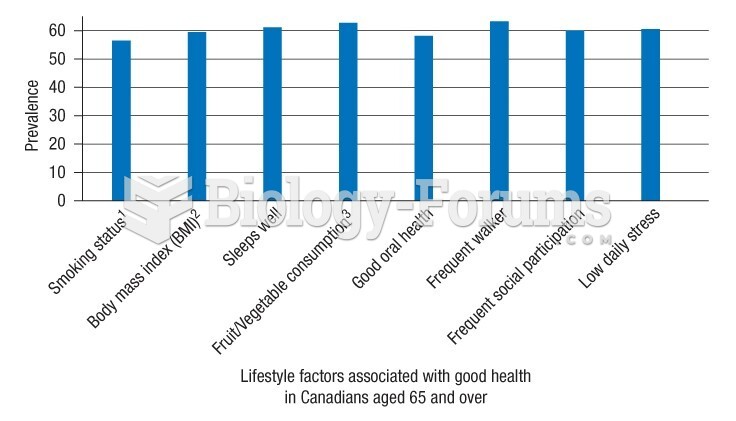 Prevalence of good health in Canadians aged 65 years and older
Prevalence of good health in Canadians aged 65 years and older