Answer to Question 1
ANS: C
Presbycusis is impaired hearing due to the aging process. Adaptation for a sensory deficit indicates that the patient alters behavior to accommodate for the sensory deficit, such as turning the unaffected ear toward the speaker. Cleaning the eye and applying spices to food would not have an effect for a patient with presbycusis. Avoiding others because of a sensory deficit is maladaptive.
Answer to Question 2
ANS: A, B, C, E
Changing positions is important for decreasing the pressure associated with long periods of time in the same position. If the patient is able to feel heat or cold and is mobile, she can protect herself by withdrawing from the source. Knowing toileting habits and any potential for incontinence is important because urine and feces in contact with the skin for long periods can increase skin breakdown. Knowing whether the patient has problems with painful movement will alert the nurse to any potential for decreased movement and increased risk for skin breakdown. Medications and falling are safety risk questions.

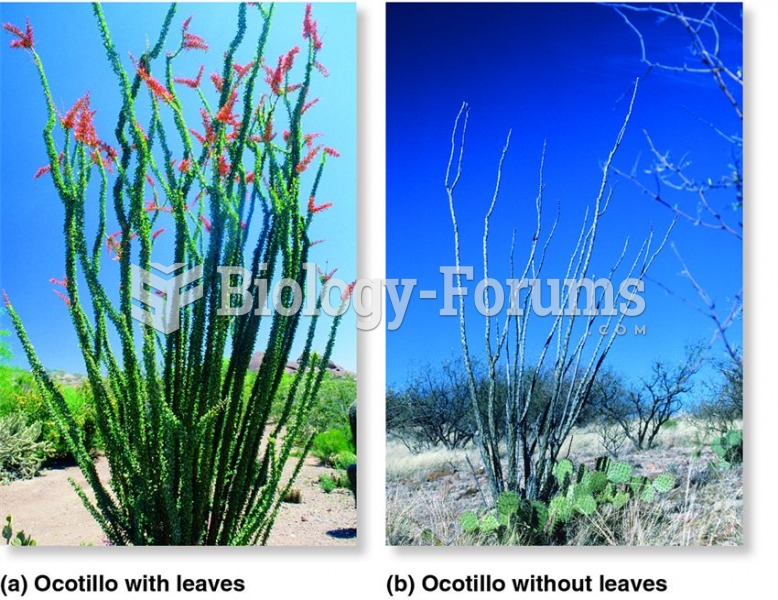 Leaf abscission as a drought adaptation.
Leaf abscission as a drought adaptation.
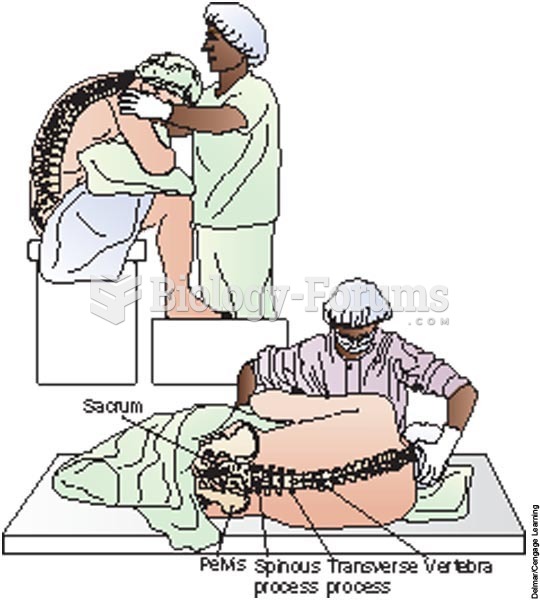 The surgical nurse assists the client into the correct position
The surgical nurse assists the client into the correct position
 Patient with a cerebrovascular accident.
Patient with a cerebrovascular accident.
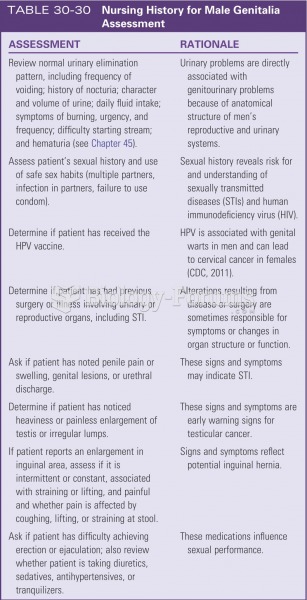 Nursing history for male genetalia assessment
Nursing history for male genetalia assessment
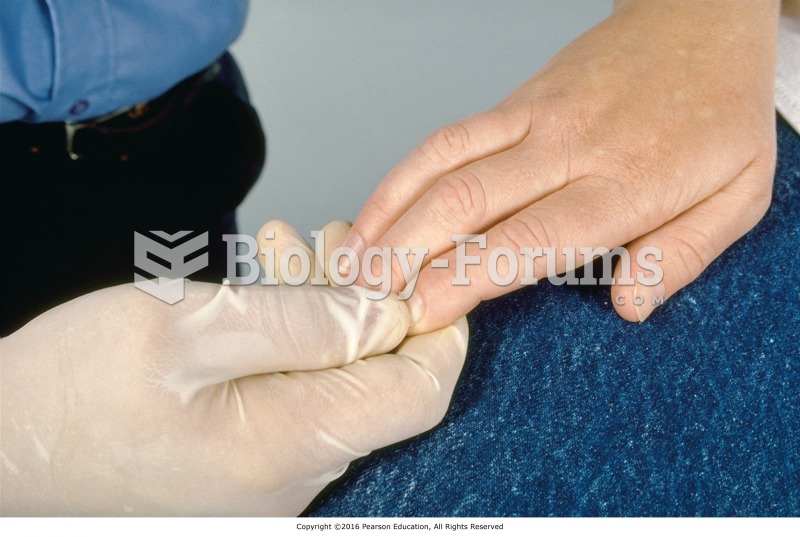 Clinician performing capillary refill assessment.
Clinician performing capillary refill assessment.
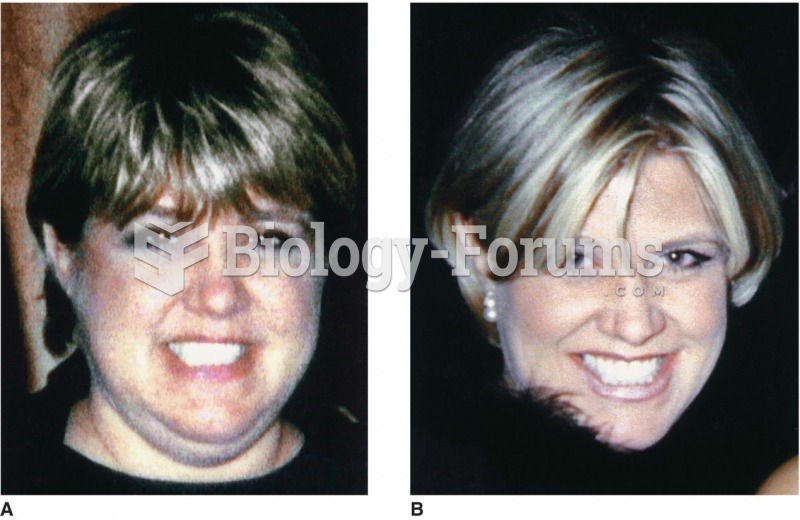 A patient with Cushing’s syndrome (A) before and (B) after receiving treatment. Sharmyn McGraw
A patient with Cushing’s syndrome (A) before and (B) after receiving treatment. Sharmyn McGraw