Answer to Question 1
ANS: B
To stimulate micturition, the nurse should attempt noninvasive procedures first. Running warm water or stroking the inner aspect of the upper thigh promotes sensory perception that leads to urination. A patient should not be left alone on a bedpan for 30 minutes because this could cause skin breakdown. Catheterization places the patient at increased risk of infection and should not be the first intervention attempted. Diuretics are useful if the patient is not producing urine, but they do not stimulate micturition.
Answer to Question 2
ANS: C
Placing the drainage bag on the side rail of the bed could allow the bag to be raised above the level of the bladder and urine to flow back into the bladder. The urine in the drainage bag is a medium for bacteria; allowing it to reenter the bladder can cause infection. A key intervention to prevent catheter-associated urinary tract infections is prevention of urine back flow from the tubing and bag into the bladder. All the rest are correct procedures and do not require follow-up. The drainage bag should be emptied when half full; an overfull drainage bag can create tension and pulling on the catheter, resulting in trauma to the urethra and/or urinary meatus and increasing risk for urinary tract infections. Urine specimens are obtained by temporarily kinking the tubing; a prolonged kink could lead to bladder distention. Failure to secure the catheter to the patient's thigh places the patient at risk for tissue injury from catheter dislodgment.

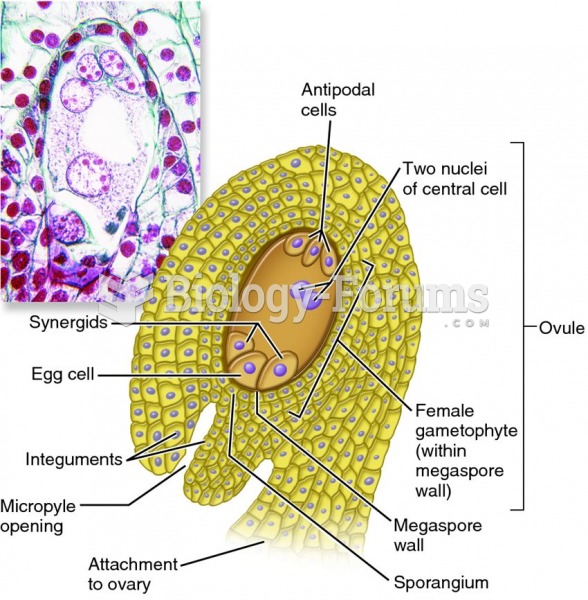 Female gametophyte within an ovule
Female gametophyte within an ovule
 The nurse needs to note the source of the patient health history
The nurse needs to note the source of the patient health history
 A pharmacist can explain to a patient why medication may look different and ensure the correct ...
A pharmacist can explain to a patient why medication may look different and ensure the correct ...
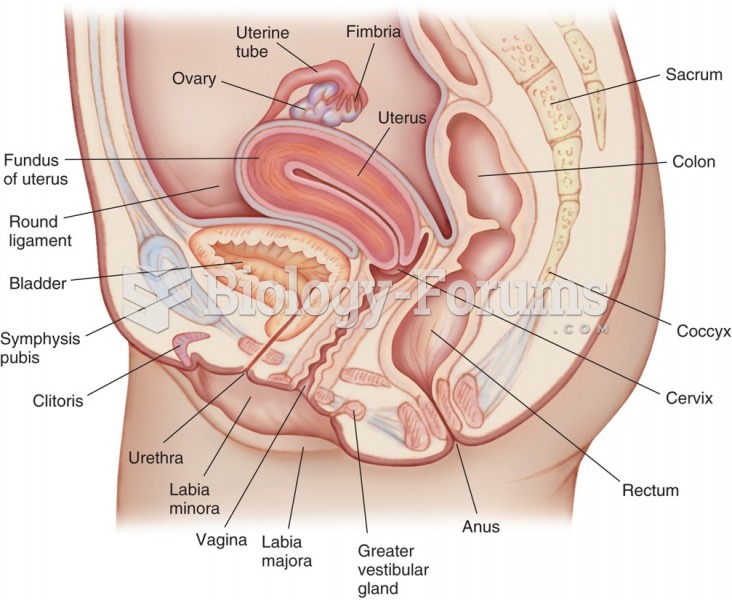 Sagittal section of the female pelvis, showing organs of the reproductive system.
Sagittal section of the female pelvis, showing organs of the reproductive system.
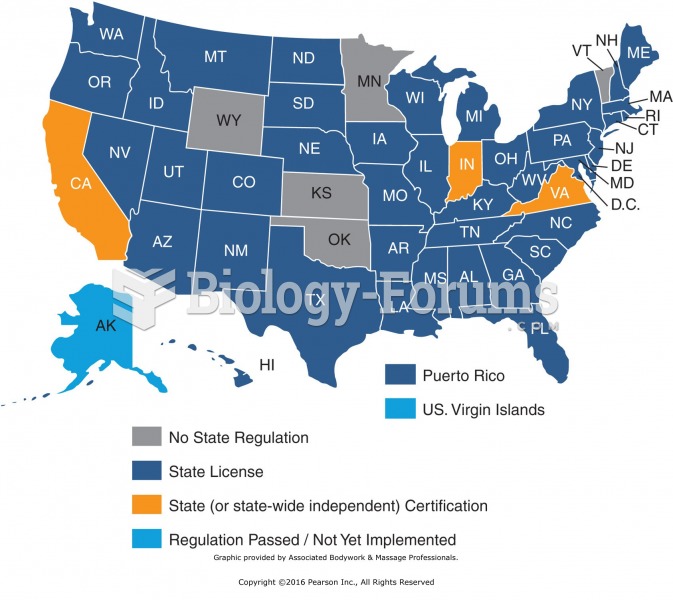 States that require licensing or certification. Graphic provided by Associated Bodywork & ...
States that require licensing or certification. Graphic provided by Associated Bodywork & ...
 Female Reproductive System "الجهاز التناسلي للأنثى"
Female Reproductive System "الجهاز التناسلي للأنثى"