Answer to Question 1
Correct Answer: 2
Rationale 1: Restlessness is observable so it is not an example of subjective data.
Rationale 2: Subjective data can be described or verified only by that person and are apparent only to the person affected. Subjective data include the client's sensations, feelings, beliefs, attitudes, and perceptions of personal health status and life situations.
Rationale 3: Not being talkative is observable so it is not an example of subjective data.
Rationale 4: Paleness with diaphoresis iare observable so it is not an example of subjective data.
Answer to Question 2
Correct Answer: 1
Rationale 1: Assessment is the collection, organization, validation, and documentation of data. Assessment is carried throughout the nursing process, as in this case. Even though performing the dressing change is implementation, noticing the new skin breakdown is assessment.
Rationale 2: Diagnosis is identifying the client's response to the problem. Implementation is what the nurse does to help the client reach a goal, and then the goal is evaluated.
Rationale 3: Even though performing the dressing change is implementation, noticing the new skin breakdown is assessment.
Rationale 4: The goal of the intervention is evaluated but that is not what is being described in this item..

 The nurse needs to note the source of the patient health history
The nurse needs to note the source of the patient health history
 Taking a Patient’s Axillary Temperature
Taking a Patient’s Axillary Temperature
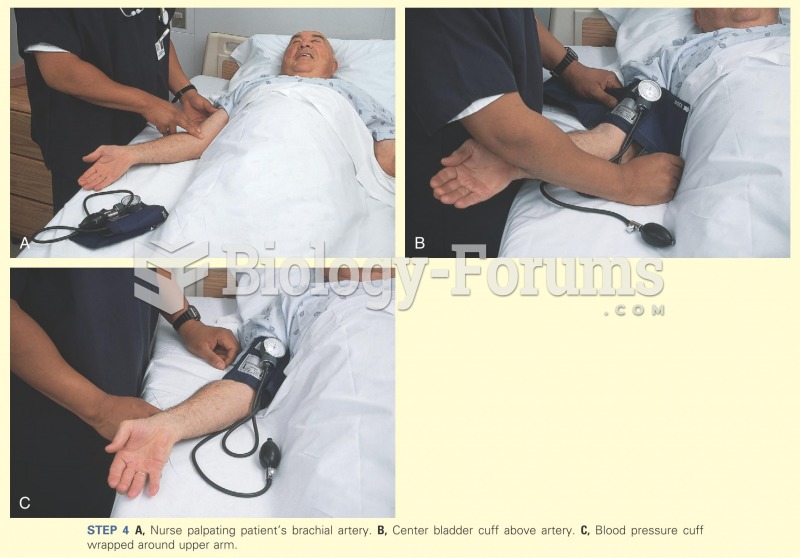 Nurse palpating the patient's brachial artery
Nurse palpating the patient's brachial artery
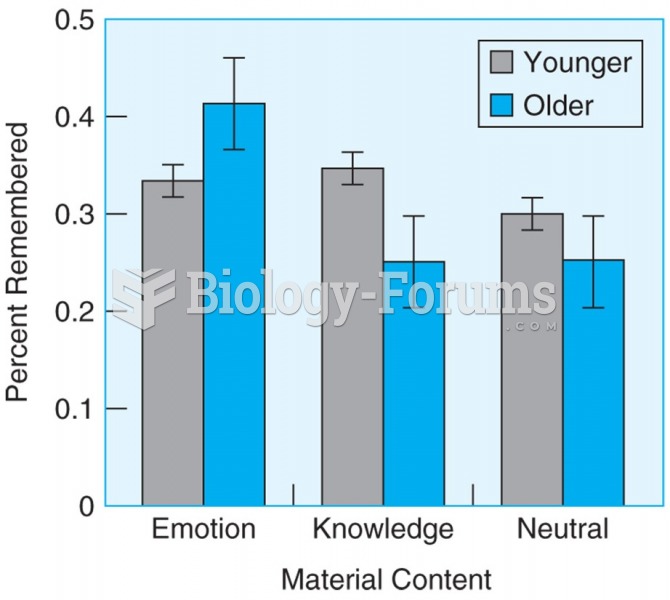 Older participants remember more information than younger participants when material has emotional ...
Older participants remember more information than younger participants when material has emotional ...
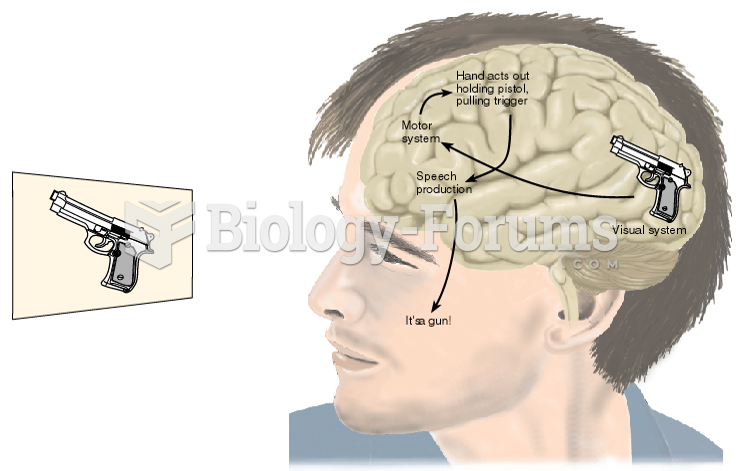 Hypothetical Exchanges of Information within the Brain of a Patient with Visual Agnosia
Hypothetical Exchanges of Information within the Brain of a Patient with Visual Agnosia
 Milk Label Containing Information about the Use of rBGH
Milk Label Containing Information about the Use of rBGH