This topic contains a solution. Click here to go to the answer
|
|
|

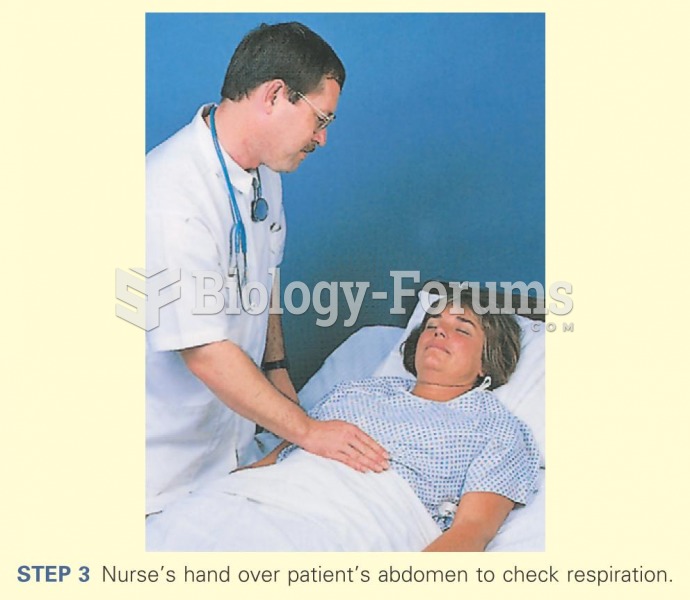 Nurse's hand over patients abdomen
Nurse's hand over patients abdomen
 Preparing Slides
Preparing Slides
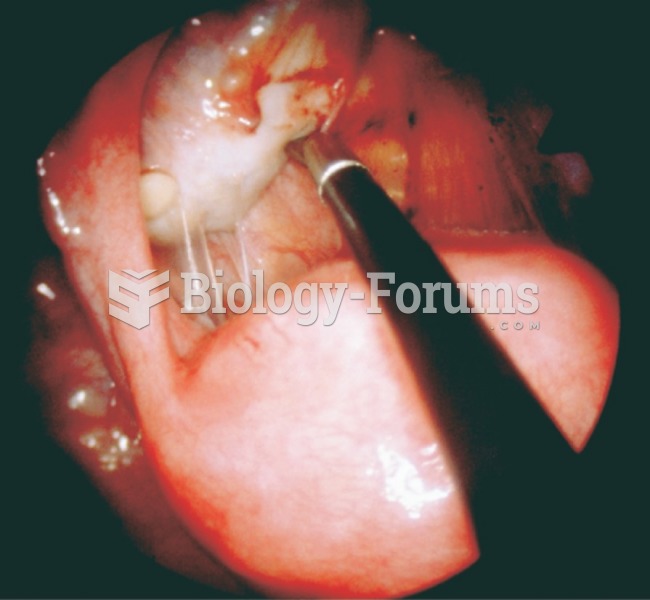 Photograph taken during a laparoscopic procedure. The uterus is visible below the probe, the ovary ...
Photograph taken during a laparoscopic procedure. The uterus is visible below the probe, the ovary ...
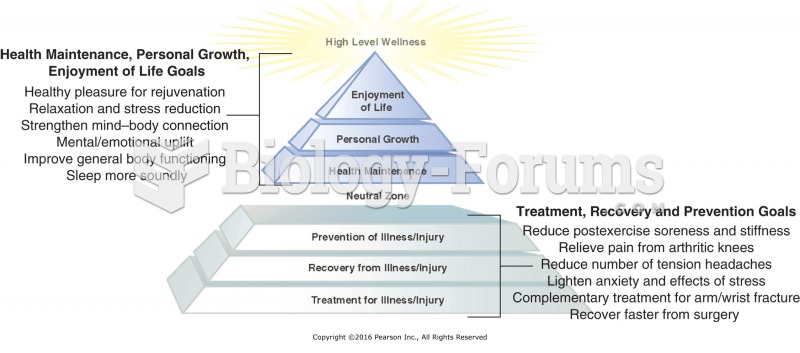 Sample client goals from the Wellness Massage Pyramid.
Sample client goals from the Wellness Massage Pyramid.
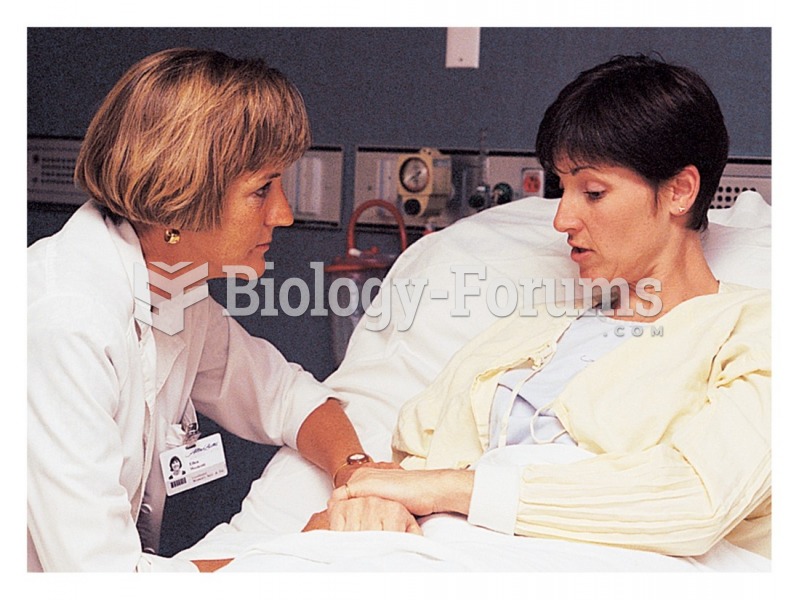 The nurse conveys attentive listening through a posture of involvement
The nurse conveys attentive listening through a posture of involvement
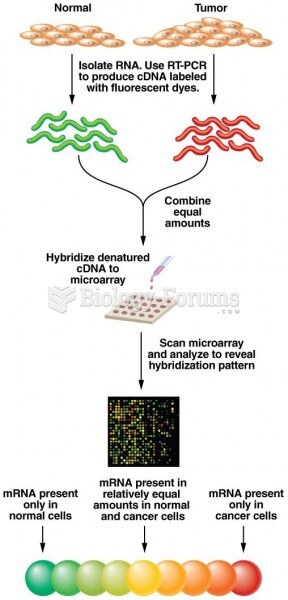 Microarray procedure for analyzing gene expression in normal and cancer cells
Microarray procedure for analyzing gene expression in normal and cancer cells