Answer to Question 1
ANS: B
After a change in the patient's condition or an untoward event, the nurse attempts to identify factors interfering with goal achievement. In this case, the nurse identifies factors that interfered with goal achievement to determine the cause of the fall. The fall may not have been due to an error by the nursing assistant; therefore, counseling should be reserved until after the cause has been determined. The patient remains a fall risk, so the fall risk sign should remain on the door. The nurse witnessing the fall or the nurse assigned to the patient needs to complete the documentation. The charge nurse can be consulted to review the documentation.
Answer to Question 2
ANS: D
The identified nursing diagnosis is Acute confusion. The outcome for this diagnosis would address a decrease or absence of confusion. One sign of orientation is when a patient responds to questions appropriately. Thus, one possible sign that a patient's confusion is improving is seen when a patient can correctly state the names of family members in the room. Keeping the side rails up and using a bed alarm are interventions to promote patient safety and prevent falls. The patient's denying pain indicates positive progress toward resolving a diagnosis of Acute or Chronic pain. The patient's wandering the halls is a sign of confusion.

 C, A nurse can also administer the medication by setting the dose and rate with an electronic infusi
C, A nurse can also administer the medication by setting the dose and rate with an electronic infusi
 NANDA international nursing diagnosis 2
NANDA international nursing diagnosis 2
 Focus on older adults - risk for infection
Focus on older adults - risk for infection
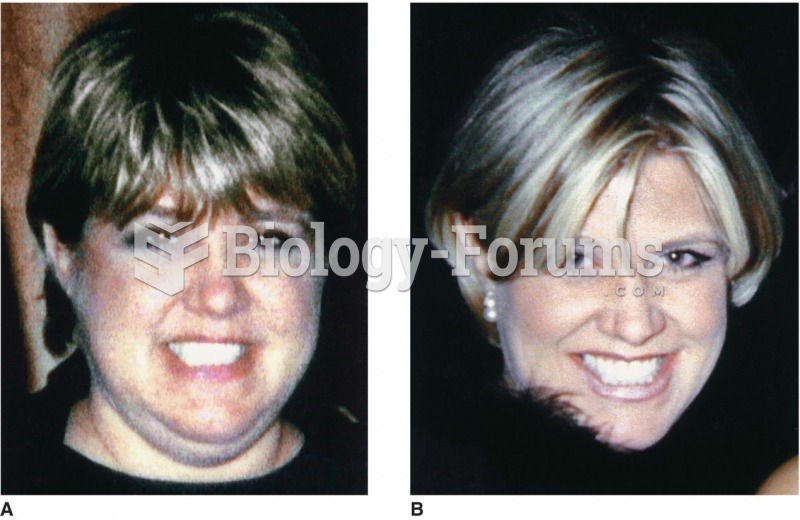 A patient with Cushing’s syndrome (A) before and (B) after receiving treatment. Sharmyn McGraw
A patient with Cushing’s syndrome (A) before and (B) after receiving treatment. Sharmyn McGraw
 Risk of Down Syndrome (Trisomy 21) by Maternal Age
Risk of Down Syndrome (Trisomy 21) by Maternal Age