Answer to Question 1
ANS: C
A medication administration record (MAR) is a list of ordered medications, along with dosages and times of administration, on which the nurse initials medications given or not given. A paper MAR usually includes a signature section in which the nurse is identified by linking the initials used with a full signature. The EHR includes an electronic medication administration record (eMAR). Flow sheets and checklists may be used to document routine care and observations that are recorded on a regular basis, such as vital signs, and intake and output measurements. Data collected on flow sheets may be converted to a graph, which pictorially reflects patient data. Originally, the Kardex was a non-permanent filing system for nursing records, orders, and patient information that was held centrally on the unit. Although computerization of records may mean that the Kardex system is no longer active, the term kardex continues to be used generically for certain patient information held at the nurses' station. An admission summary includes the patient's history.
Answer to Question 2
ANS: D
Charting by exception (CBE) is documentation that records only abnormal or significant data. A PIE note is used to document problem (P), intervention (I), and evaluation (E). A SOAP note is used to chart the subjective data (S), objective data (O), assessment (A), and plan (P). Narrative charting is chronologic, with a baseline recorded on a shift-by-shift basis. Data are recorded in the progress notes, often without an organizing framework. Narrative charting may stand alone, or it may be complemented by other tools.

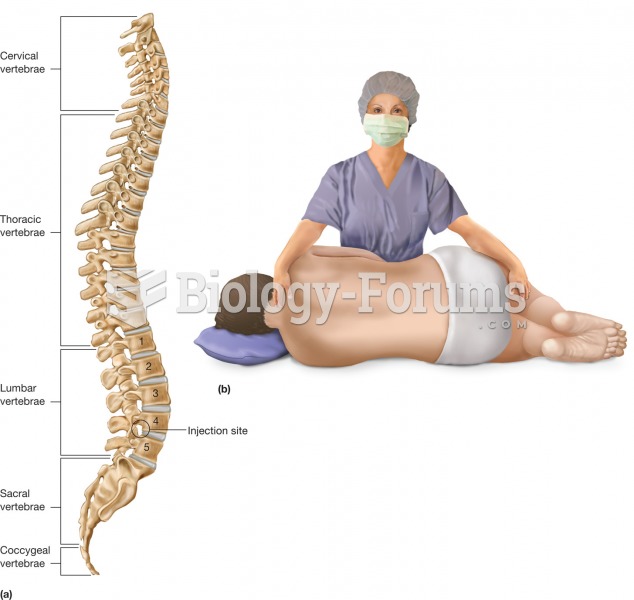 Lumbar puncture. Abbreviated LP, the lumbar puncture is a common procedure that withdraws cerebrospi
Lumbar puncture. Abbreviated LP, the lumbar puncture is a common procedure that withdraws cerebrospi
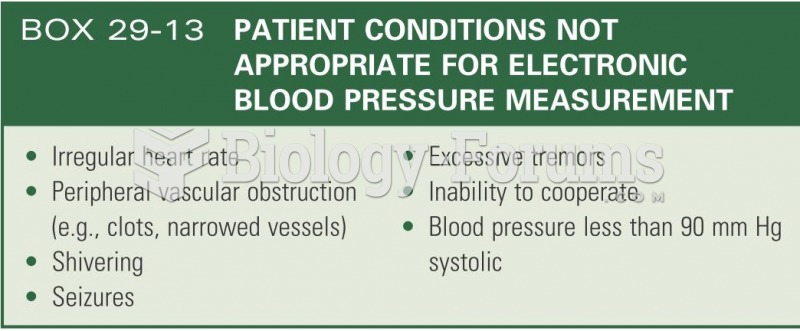 Patient conditions not appropriate for elctronic blood pressure measurement
Patient conditions not appropriate for elctronic blood pressure measurement
 Calibrated cups, spoons, droppers, and syringes are often used to administer liquid medications.
Calibrated cups, spoons, droppers, and syringes are often used to administer liquid medications.
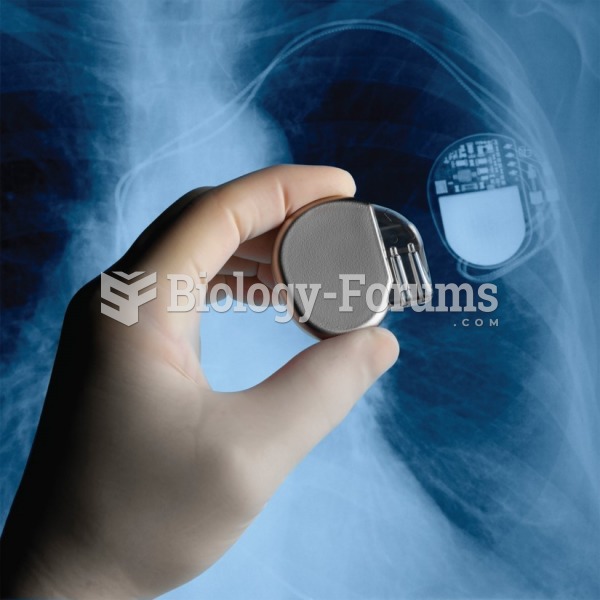 A surgeon holds a pacemaker next to an X-ray of a pacemaker implanted in a patient’s chest.
A surgeon holds a pacemaker next to an X-ray of a pacemaker implanted in a patient’s chest.
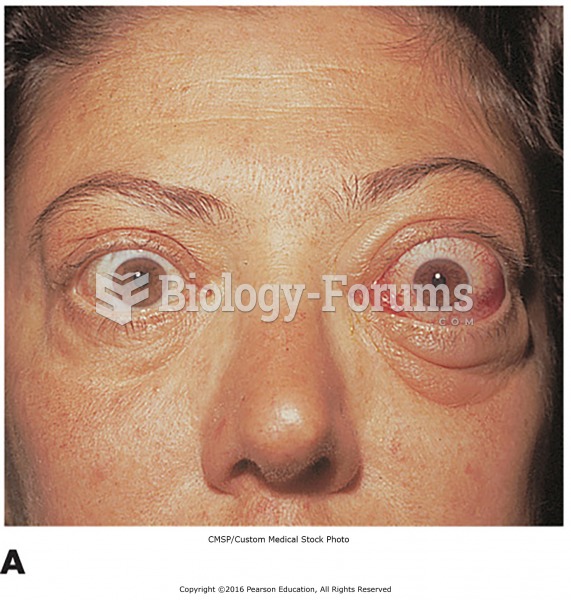 Examples of endocrine disorders. (A) A patient with exophthalmos, a symptom of hyperthyroidism ...
Examples of endocrine disorders. (A) A patient with exophthalmos, a symptom of hyperthyroidism ...
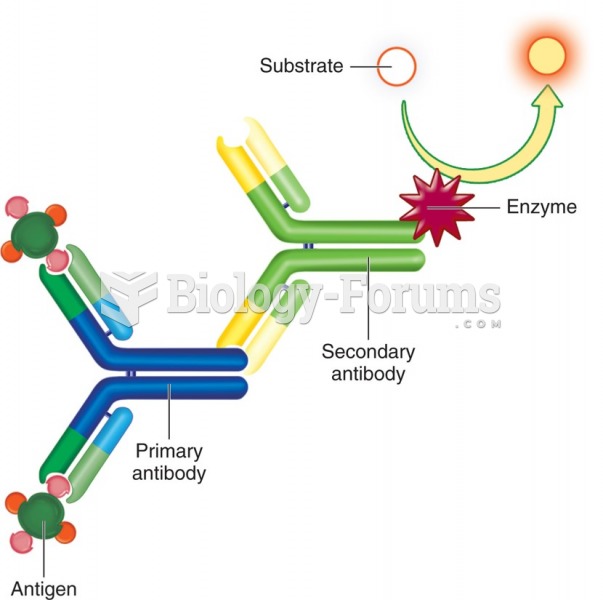 Indirect enzyme immunoassay. A patient's antibody reacts with the antigen, which is detected ...
Indirect enzyme immunoassay. A patient's antibody reacts with the antigen, which is detected ...