Answer to Question 1
The strategies that therapists use today in treating DID are based on accumulated clinical wisdom. The fundamental goal is to identify cues or triggers that provoke memories of trauma, dissociation, or both and to neutralize them. More important, the patient must confront and relive the early trauma and gain control over the horrible events, at least as they recur in the patient's mind. To instill this sense of control, the therapist must skillfully, and slowly, help the patient visualize and relive aspects of the trauma until it is simply a terrible memory instead of a current event. Because the memory is unconscious, aspects of the experience are often not known to either the patient or the therapist until they emerge during treatment. Hypnosis is often used to access unconscious memories and bring various alters into awareness. Because the process of dissociation may be similar to the process of hypnosis, the latter may be a particularly efficient way to access traumatic memories. DID seems to run a chronic course and seldom improves spontaneously, which confirms that current treatments, primitive as they are, have some effectiveness.
Answer to Question 2
Conversion disorders
generally have to do with physical malfunctioning, such as paralysis, blindness, or difficulty speaking (aphonia), without any physical or organic pathology to account for the malfunction. Most conversion symptoms suggest that some kind of neurological disease is affecting sensorymotor systems, although conversion symptoms can mimic the full range of physical malfunctioning. For this reason, and because the term conversion implies a specific etiology for which there is limited evidence, the name changed to functional neurological disorder (with functional referring to a symptom without organic cause) in the DSM-5..
Conversion disorders provide some of the most intriguing, sometimes astounding, examples of psychopathology. What could possibly account for somebody going blind when all visual processes are normal, or experiencing paralysis of the arms or legs when there is no neurological damage? Conversion symptoms are often precipitated by marked stress. C.V. Ford (1985) noted that the incidence of marked stress preceding a conversion symptom occurred in 52 to 93 percent of the studied patients. Often, this stress takes the form of a physical injury. In one large survey, 324 out of 869 patients (37 percent) reported prior physical injury. Thus, if the clinician cannot identify a stressful event preceding the onset of the conversion symptom, the clinician might more carefully consider the presence of a true physical condition.
In addition, although people with conversion symptoms can usually function normally, they seem truly unaware either of this ability or of sensory input. For example, individuals with the conversion symptom of blindness can usually avoid objects in their visual field, but they will tell you they can't see the objects. Similarly, individuals with conversion symptoms of paralysis of the legs might suddenly get up and run in an emergency and then be astounded they were able to do this. It is possible that at least some people who experience miraculous cures during religious ceremonies may have been suffering from conversion reactions. These factors may help in distinguishing between conversion and organically based physical disorders, but clinicians sometimes make mistakes, although it is not common with modern diagnostic techniques. In any case, ruling out medical causes for the symptoms is crucial to making a diagnosis of conversion.

 Bipolar disorder.
Bipolar disorder.
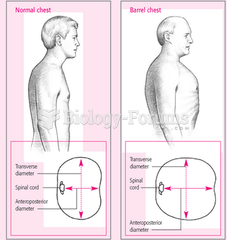 Barrel Chest for Patients who have COPD
Barrel Chest for Patients who have COPD
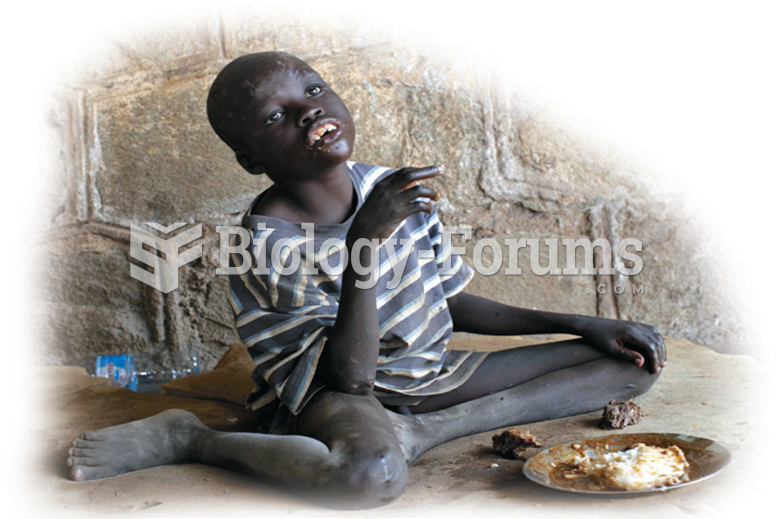 A child in an orphanage in Juba, Sudan. The treatment of this child is likely to affect his ability ...
A child in an orphanage in Juba, Sudan. The treatment of this child is likely to affect his ability ...
 Botox therapy: (left) before treatment; (right) after treatment.
Botox therapy: (left) before treatment; (right) after treatment.
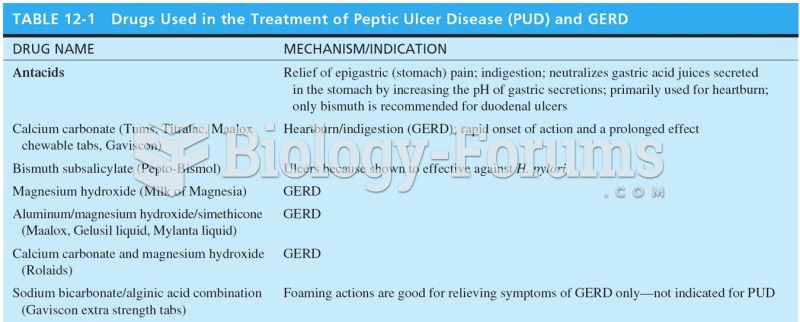 Drugs Used in the Treatment of Peptic Ulcer Disease (PUD) and GERD
Drugs Used in the Treatment of Peptic Ulcer Disease (PUD) and GERD
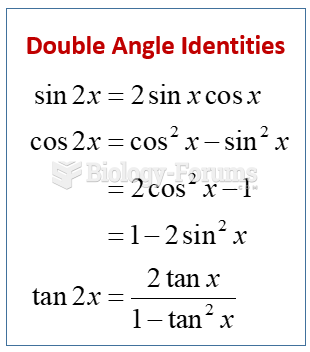 Double Angle Identity
Double Angle Identity