Answer to Question 1
The life-course-persistent (LCP) path describes children who engage in aggression and antisocial behavior at an early age and continue to do so into adulthood (Moffitt et al., 1996). They may display biting and hitting at age 4, shoplifting and truancy at age 10, selling drugs and stealing cars at age 16, robbery and rape at age 22, and fraud and child abuse at age 30 (Moffitt, 1993, p. 679). Their underlying disposition remains, but the way it is expressed changes with new opportunities at different points in development. For these children, antisocial behavior begins early because of subtle neuropsychological deficits that may interfere with their development of language, memory, and self-control, resulting in cognitive deficits and a difficult temperament by age 3 or younger. The adolescent-limited (AL) path describes youths whose antisocial behavior begins around puberty and continues into adolescence, but who later cease these behaviors during young adulthood. This path includes most juvenile offenders whose antisocial behavior is limited primarily to their teen years (Hamalainen & Pulkkinen, 1996). Teens on the AL path display less extreme antisocial behavior than those on the LCP path, are less likely to drop out of school, and have stronger family ties. Their delinquent activity is often related to temporary situational factors, especially peer influences. The behavior of AL youths is not consistent across situations; they may use drugs or shoplift with their friends while continuing to follow rules and to do well in school. Although these children do not display antisocial behavior in childhood, they do experience, like youngsters on the LCP path, greater social adversity and personal risk during childhood relative to other youths, suggesting that the AL pathway is not simply part of normal adolescent development (Roisman et al., 2010).
Answer to Question 2
The earliest indications of conduct problems may be a difficult temperament in the first few years of life, expressed as fussiness, irritability, irregular sleeping and eating patterns, or fearfulness in response to novel events. During the preschool and early school years, a child with a difficult temperament displays an increase in hyperactivity and impulsivity with growing mobility, weak emotion-regulation skills, and a heightened risk for simple forms of oppositional and aggressive behaviors that peak during the preschool years (Tremblay, 2000). Most children with conduct problems show diversificationthey add new forms of antisocial behavior over time rather than simply replacing old behaviors. Poor social skills and socialcognitive deficits often accompany early oppositional and aggressive behaviors, predisposing the child to poor peer relationships, rejection by peers, and social isolation and withdrawal. In this progression, we see a snowballing negative cycle over time, where one deficit or problem behavior produces direct and indirect changes in others. For example, peer rejection leads to socialcognitive deficits and aggression; socialcognitive deficits lead to peer rejection and aggression; aggression leads to peer rejection (Lansford et al., 2010). Conversely, better socialcognitive skills may increase peer acceptance and lower aggressiveness. These cascading effects highlight the importance of looking at the progression of antisocial behavior over time as a dynamic developmental process involving relationships among neurobiological dispositions, social environments, cognitions, and behavior (Lansford et al., 2010).

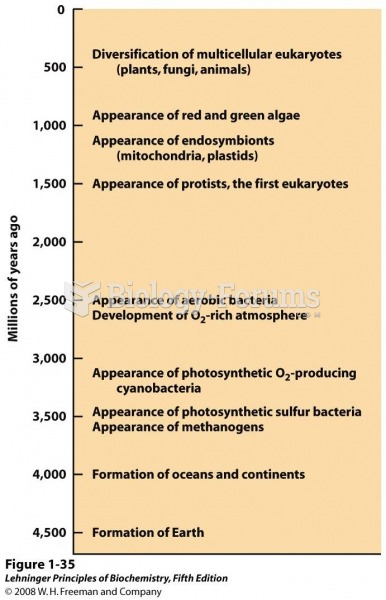 Landmarks in the evolution of life on Earth
Landmarks in the evolution of life on Earth
 Two stubby screwdrivers used to access screws that have limited space above. A straight blade is on ...
Two stubby screwdrivers used to access screws that have limited space above. A straight blade is on ...
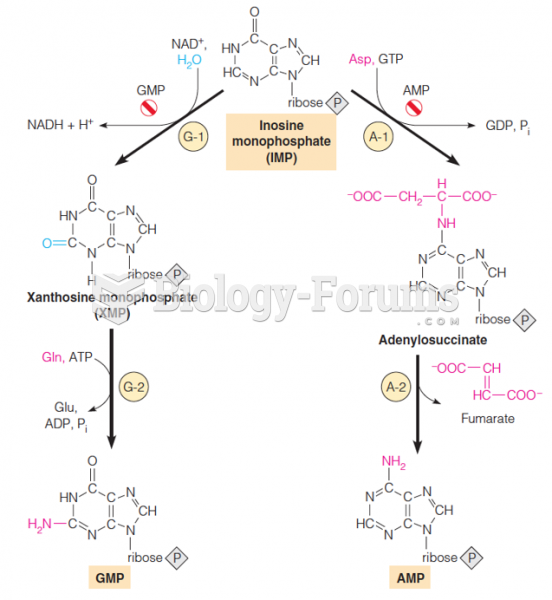 Pathways from IMP to GMP and AMP
Pathways from IMP to GMP and AMP
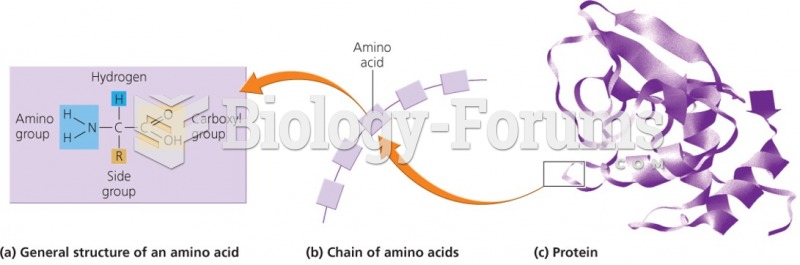 Macromolecules and the building blocks of life
Macromolecules and the building blocks of life
 Gene action in pathways
Gene action in pathways
 Oxidative stress can begin in childhood and lead to progressive damage throughout life
Oxidative stress can begin in childhood and lead to progressive damage throughout life