PROCEDURE REPORT
INDICATIONS: 55-year-old male with episodic abdominal pain for almost a year. Recurrence of the pain ultimately led to cholecystectomy in 8-90. Periodically the pain has been severe enough that he goes to the emergency room. I have seen him in the past for left upper quadrant pain, which I felt, was due to irritable bowel syndrome. Four days ago, he had an episode of severe epigastric pain that seemed to radiate up into his chest and at times his neck. He described the pain as burning. It lasted a few hours and then resolved. Last night the pain recurred and was extremely severe. He was taken to the emergency room where he required parenteral narcotics.
PROCEDURE: Following informed consent , he was sedated with Demerol 40 mg and Versed 1 mg IV. Oropharyngeal anesthesia with Cetacaine spray was administered. An Olympus OES type GIF-XQlO endoscope was introduced. The esophagus was unremarkable. The z-line was at 40 cm. from the incisors. There was no endoscopic esophagitis. No hiatal hernia was seen. Retroflex exam of the fundus and cardia was unrevealing. Pylorus , duodenal bulb, and several centimeters of post-bulbar duodenum were also unremarkable. The ampulla of Vater was seen tangentially and normal. He tolerated the procedure well. Two biopsies were taken of the distal esophagus to look for histologic evidence of inflammation.
IMPRESSION: Normal esophagogastroduodenoscopy. Wonder if he is having panic attacks. He does describe some symptoms of gastroesophageal reflux disease and irritable bowel syndrome as noted above.
PLAN: He will be discharged to home and will remain on Zantac 105 mg po bid. I will notify him with the biopsy reports. He will try Xanax 0.5 mg po at the onset of pain in the future. He is aware that this may cause sedation and that he should be careful around moving vehicles.
ICD-9-CM diagnosis code(s): _____________________
ICD-10-CM diagnosis code(s): _____________________
CPT code(s) with modifier, if applicable: _____________________

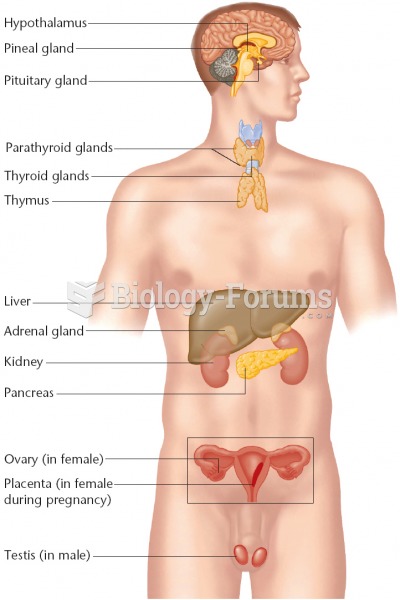 Endocrine System - male
Endocrine System - male
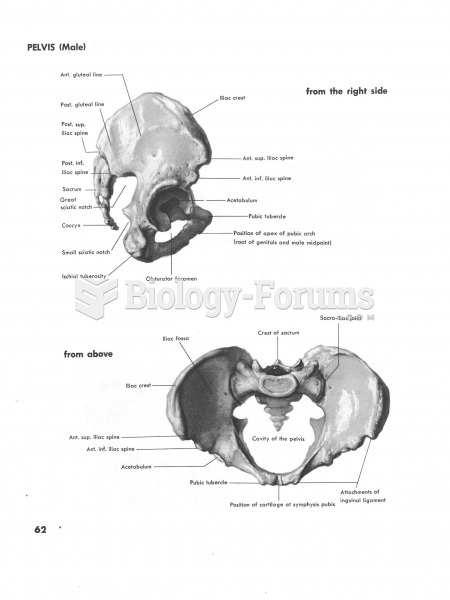 Pelvis Male from side and above
Pelvis Male from side and above
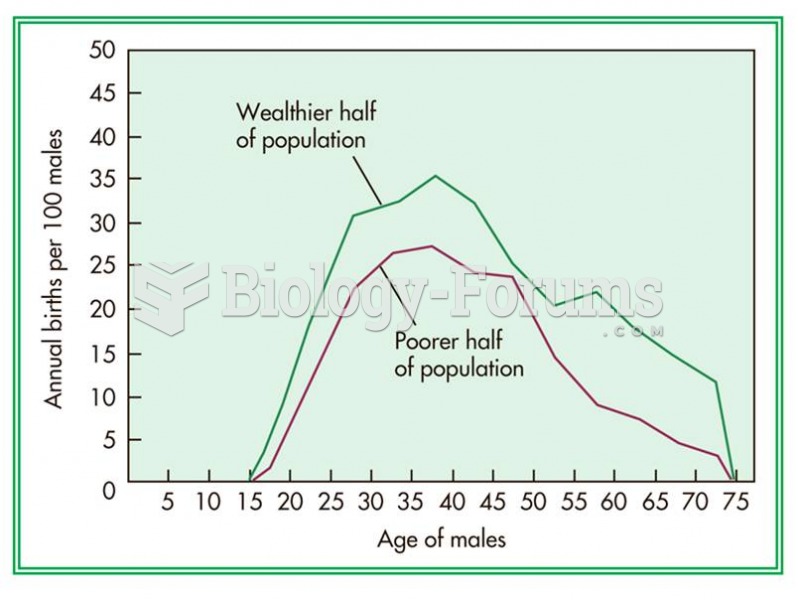 Male Turkmen in the wealthier half of the population had higher fertility rates than those in the po
Male Turkmen in the wealthier half of the population had higher fertility rates than those in the po
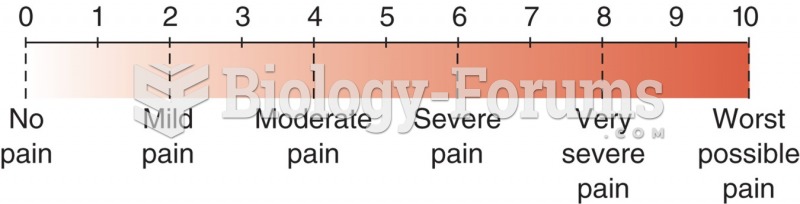 Numerical pain level chart with word modifiers.
Numerical pain level chart with word modifiers.
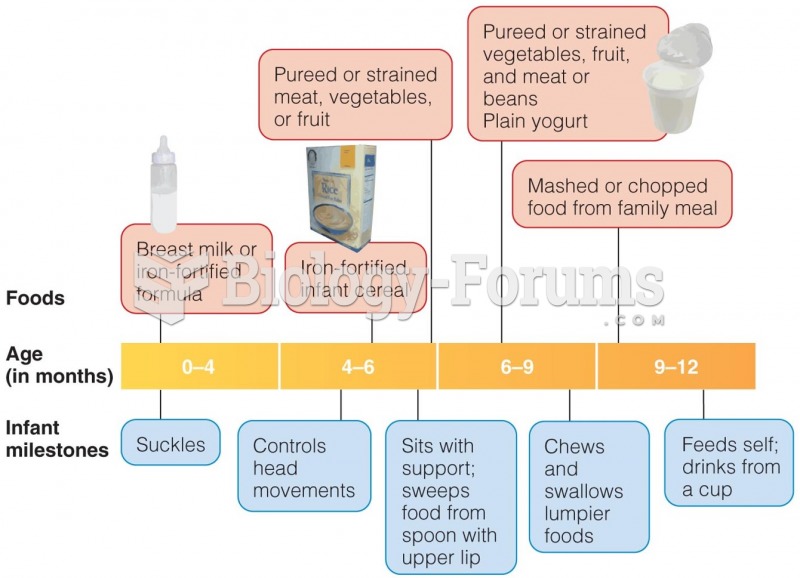 Foods for Baby’s First Year
Foods for Baby’s First Year
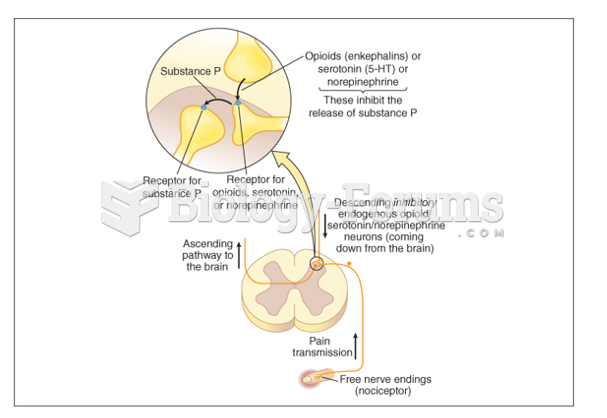 Neural pathways for pain
Neural pathways for pain