Answer to Question 1
ANS: C
One of the key factors in tracking malnutrition is measuring and recording clients' heights and weights. Most adults overestimate their height and underestimate their weight on self-report; height is a particular problem because adults tend to lose 1 inch of height every 20 years after age 35 to 40. Measurement of standing height is difficult if there is any degree of kyphosis (underestimates the actual height).
Answer to Question 2
ANS: C
Older adults are increasingly turning to exercise for socialization and fitness, and this trend should be supported. The question always arises: How much screening and assessment should be conducted prior to initiating an exercise program? The Canadian Society for Exercise Physiology has developed a useful evidence-based, seven-question screening tool, the Physical Activity Readiness Questionnaire (PAR-Q) for screening adults up to age 69 (2002). The recommendation for those over age 69 who are not accustomed to being active is to consult with a health-care provider prior to initiating a formal exercise program. The questions on the PAR-Q require a yes or no response; any response of yes requires further screening by a health-care provider. There is a companion form, the PARmed-X, for the clinician to complete prior to the individual beginning a formal exercise program. The PARmed-X includes a clearance as well as suggestions for special prescriptions for conditions such as chronic obstructive pulmonary disease. There are relatively few absolute contraindications to exercise listed on the PARmed-X; they include acute infectious processes, dissecting aortic aneurysm, severe aortic stenosis, active or recent myocarditis, acute myocardial infarction or heart failure, and acute thrombotic or embolic processes. Once any acute illness is resolved, the adult should be rescreened and allowed to exercise to tolerance.

 Discipline-specific training can take years to perfect.
Discipline-specific training can take years to perfect.
 Older adults may grieve intensely over the loss of a person or situation that has been a part of the
Older adults may grieve intensely over the loss of a person or situation that has been a part of the
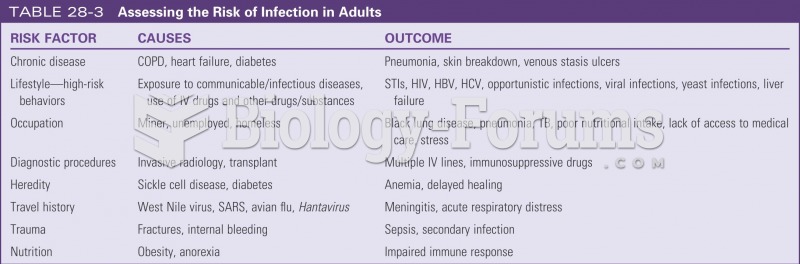 Assessing risk for infection in adults
Assessing risk for infection in adults
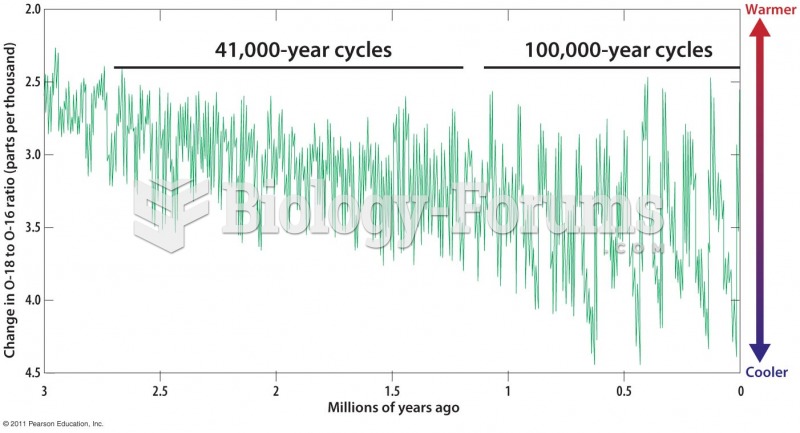 Shifts between Warm and Cold Periods during the Last 3 Million Years
Shifts between Warm and Cold Periods during the Last 3 Million Years
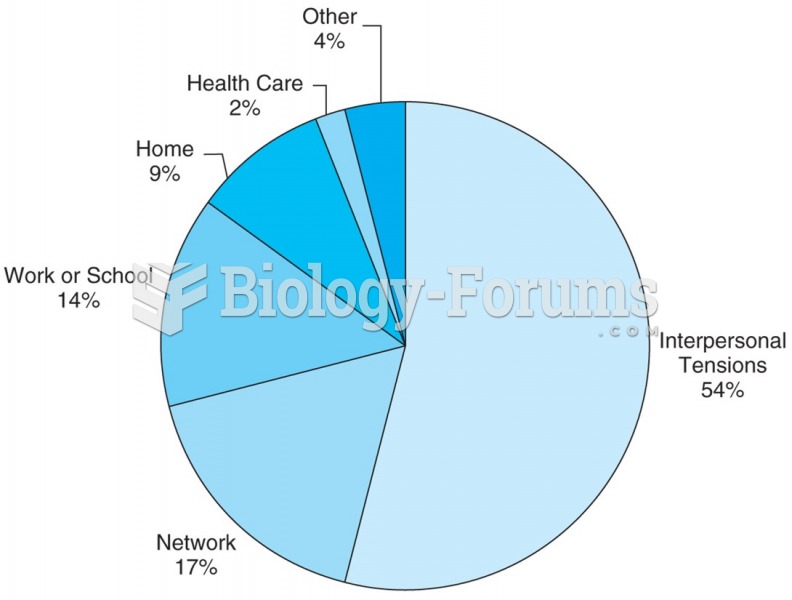 U.S. adults from 25 to 74 years report that the largest proportion of their daily stressors arise ...
U.S. adults from 25 to 74 years report that the largest proportion of their daily stressors arise ...
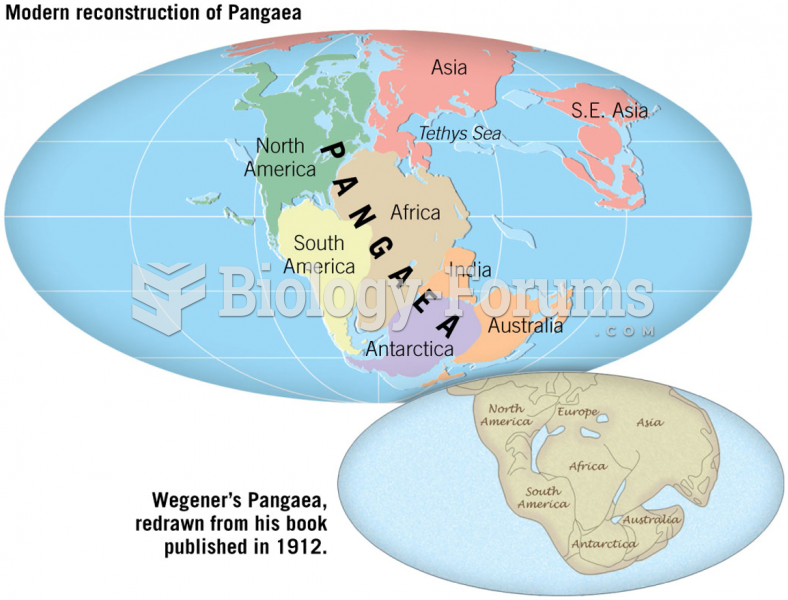 Pangaea 200 Million Years Ago
Pangaea 200 Million Years Ago