Answer to Question 1
Correct Answer: 3
The UAP can safely be taught to report complaints of pain or leakage from an IV site if it is noted during routine care, but the UAP is not responsible for assessing the site, because the nurse is responsible for all assessments. The IV dressing should be changed using sterile technique, and should not be delegated to the UAP. Whether medications are added to the IV fluid or not, only the nurse can change the bag, because sterile technique is required, and even a plain solution is considered a medication.
Answer to Question 2
Correct Answer: 1,2,3,4
Central venous access can be very useful for clients requiring long-term IV therapy because the catheter can remain in place for extended periods, and IV sites do not have to be changed every few days. Caustic medications are less likely to cause phlebitis when administered into the large central veins as opposed to the smaller peripheral veins. In the critical care areas where clients may receive numerous continuous IV medication drips that might not all be compatible infusing through the same site, a multiple-port central venous access device can provide the best option. Clients who are unstable and require rapid administration of medications require reliable IV access that might not be available with peripheral IV lines, and central venous access may be the best option. Because of the potential complications from central venous access, it would not be an option considered because of client preference if short-term IV therapy is required.

 The nurse needs to inform the patient with impaired vision when a touch is to occur and ask permissi
The nurse needs to inform the patient with impaired vision when a touch is to occur and ask permissi
 The nurse can make observations about the patient's general appearance while talking with the p
The nurse can make observations about the patient's general appearance while talking with the p
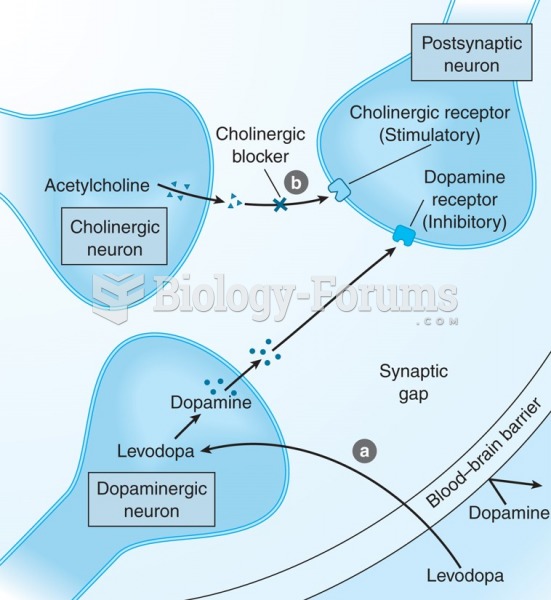 Mechanism of action of anti-parkinson drugs. (a) Levodopa therapy increases dopamine production; (b) ...
Mechanism of action of anti-parkinson drugs. (a) Levodopa therapy increases dopamine production; (b) ...
 Hands-on class in a massage therapy program.
Hands-on class in a massage therapy program.
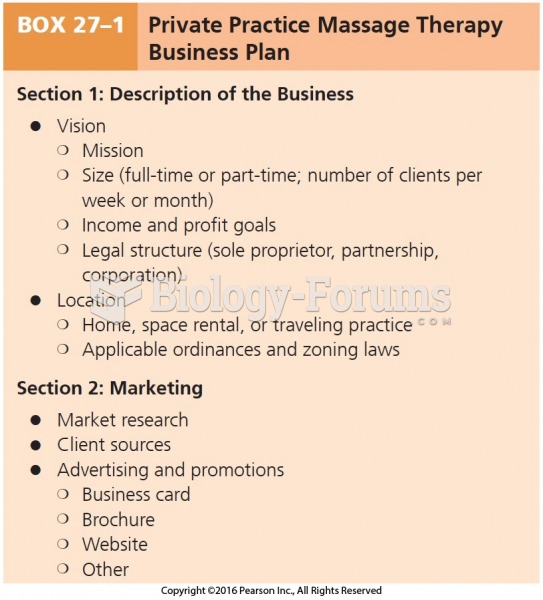 Private Practice Massage Therapy Business Plan
Private Practice Massage Therapy Business Plan
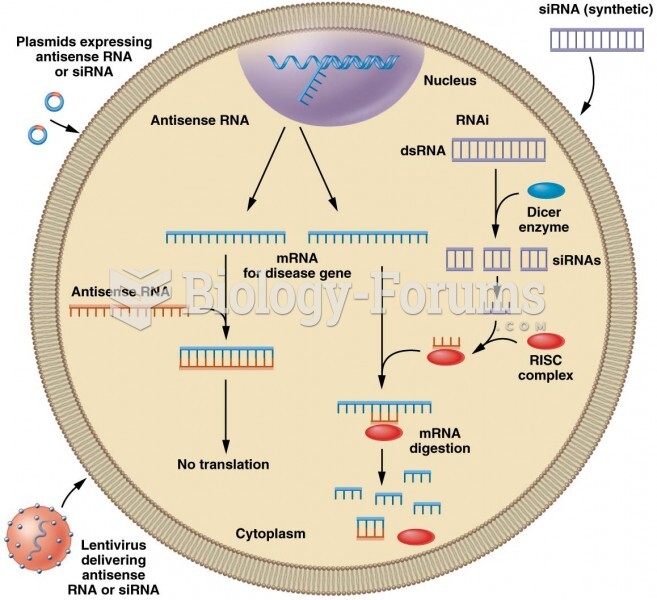 Antisense RNA and RNA interference (RNAi) approaches to silence genes for gene therapy
Antisense RNA and RNA interference (RNAi) approaches to silence genes for gene therapy