Answer to Question 1
Correct Answer: 1
The apocrine glands are dormant until the onset of puberty, when they become active and produce secretion of water, salts, fatty acids, and proteins. This secretion is released into hair follicles primarily in auxiliary and anogenital areas, and when mixed with bacteria on skin surface produces a musky odor. This is a normal part of normal growth and development. The teenage client's healthcare provider does not need to be notified because this odor is associated with normal growth and development. The nurse does not need to obtain a dietary referral because this odor is associated with normal growth and development. Increasing fluid intake will not help prevent the occurrence of this odor. It is a normal part of normal growth and development.
Answer to Question 2
Correct Answer: 3
Reddened, swollen, localized, painful areas should not be palpated because these signs and symptoms indicate the presence of inflammation and possible infection. Disturbance may spread the infection into skin layers. The healthcare provider should be notified. The nurse would not palpate the area. The nurse would not apply a heating pad to this site. The nurse would not necessarily place the client on bed rest.

 The nurse can make observations about the patient's general appearance while talking with the p
The nurse can make observations about the patient's general appearance while talking with the p
 Assessing for Bulge Sign, Observing for Fluid
Assessing for Bulge Sign, Observing for Fluid
 The nurse assesses the patient's ability to use the walker correctly
The nurse assesses the patient's ability to use the walker correctly
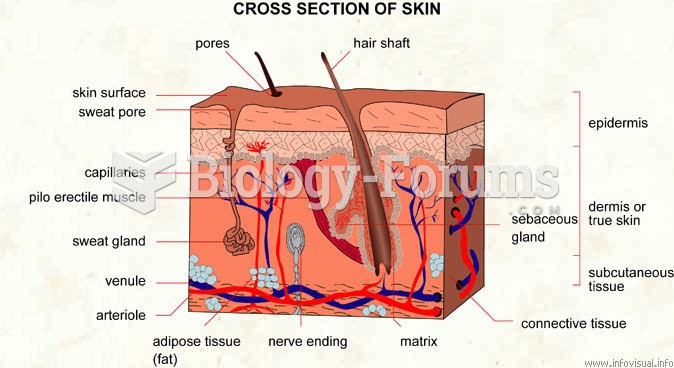 Cross section of skin
Cross section of skin
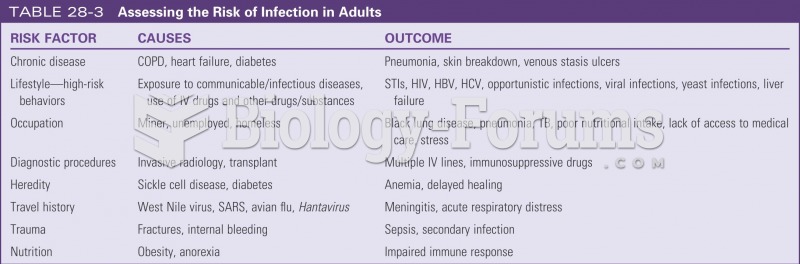 Assessing risk for infection in adults
Assessing risk for infection in adults
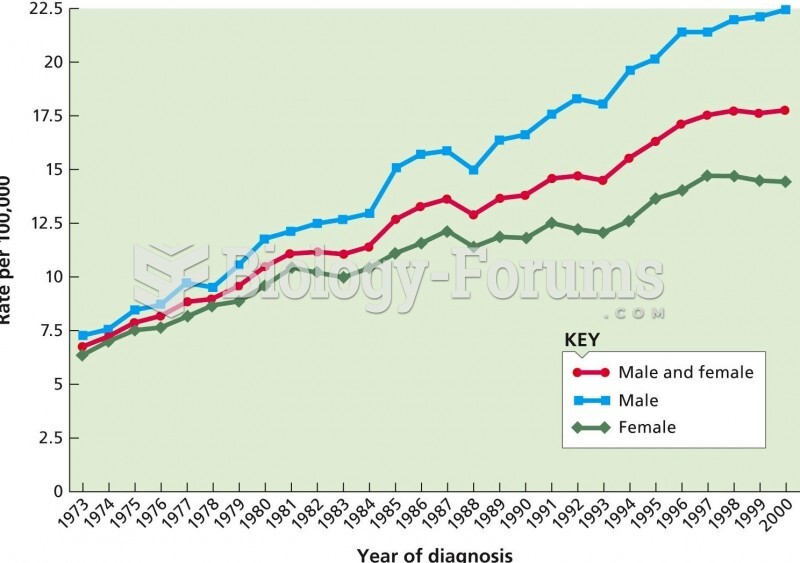 The age-adjusted rate of melanoma, a deadly form of skin cancer, from 1973 to 2000. Over that time p
The age-adjusted rate of melanoma, a deadly form of skin cancer, from 1973 to 2000. Over that time p