Answer to Question 1
ANS: B
The normal chest has a lateral diameter that is twice as large as the AP diameter. When the AP diameter approaches or exceeds the lateral diameter, the client is said to have a barrel chest. Most commonly, barrel chest occurs as a result of a long-term chronic airflow limitation problem, such as chronic obstructive pulmonary disease or severe chronic asthma. It can also be seen in people who have lived at a high altitude for many years. Therefore, an AP chest diameter that is the same as the lateral chest diameter should be rechecked but is not as indicative of underlying disease processes as an AP diameter that exceeds the lateral diameter. Medications, herbal supplements, and aerobic exercise are not associated with a barrel chest. Although occupation and hobbies may expose a client to irritants that can cause chronic lung disorders and barrel chest, asking about chronic breathing problems is more direct and should be asked first.
Answer to Question 2
ANS: C
Wheezes are indicative of narrowed airways, and bronchodilators help to open the air passages. Hollow sounds are typically heard over the trachea, and no intervention is necessary. If crackles are heard, the client may need a diuretic. Crackles represent a deep interstitial process, and coughing forcefully will not help the client expectorate secretions. Vesicular sounds heard in the periphery are normal and require no intervention.

 Pattern for Tactile Fremitus, Left Lateral Thorax
Pattern for Tactile Fremitus, Left Lateral Thorax
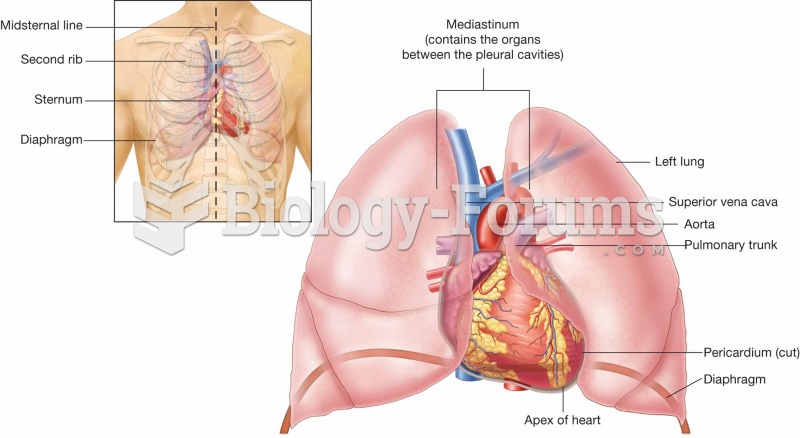 Location of the heart in the chest cavity.
Location of the heart in the chest cavity.
 Home Health Nurse.
Home Health Nurse.
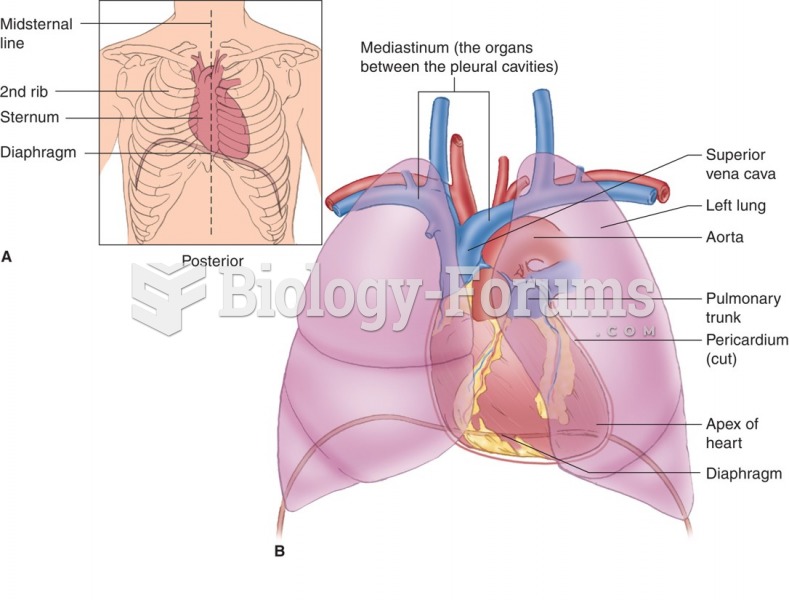 Location of the heart in the chest cavity.
Location of the heart in the chest cavity.
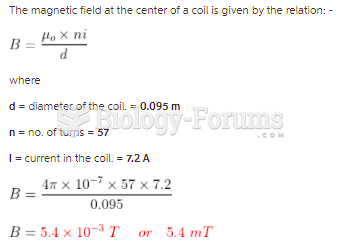 A flat circular coil having 57 turns of very thin wire has a diameter of 9.5 cm and carries 7.2 ...
A flat circular coil having 57 turns of very thin wire has a diameter of 9.5 cm and carries 7.2 ...