Answer to Question 1
ANS: A
This child appears to be experiencing a complication of fracture, which may include shock, fat embolism, deep vein thrombosis, pulmonary embolism, and infection. Shortness of breath should alert the nurse to a respiratory complication as a first priority. The nurse should have a coworker call the physician while obtaining other assessment data, including oxygen saturation, vital signs, and a respiratory assessment. Although it is possible that a postoperative hemoglobin and hematocrit are low enough that the child is experiencing shock, the priority steps in assessing and intervening are airway, breathing, and circulation (ABCs), so breathing comes before circulation. The child may have pain or anxiety, but these are not the priority. Raising the head of the bed may or may not be helpful, but the nurse first needs to assess oxygen saturation.
Answer to Question 2
ANS: A
After surgery and/or casting, it is vital to assess neurovascular status, which is usually done with postoperative vital signs. Excessive swelling can disrupt circulation to the extremity, so the nurse assesses the child's neurovascular status frequently. Applying ice is also a good intervention, but not for more than 15 minutes at a time. When the child is tolerating oral foods and fluids, the nurse can switch to pain pills from IV narcotics. Teaching is important, but not as important as preventing injury from complications.

 Open Heart Surgery
Open Heart Surgery
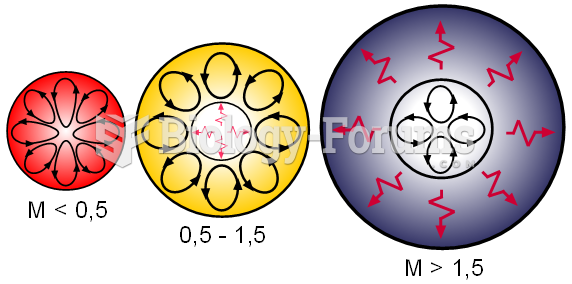 Internal structures of main sequence stars, convection zones with arrowed cycles and radiative zones
Internal structures of main sequence stars, convection zones with arrowed cycles and radiative zones
 Internal structures of main sequence stars, convection zones with arrowed cycles and radiative zones
Internal structures of main sequence stars, convection zones with arrowed cycles and radiative zones
 The Taung Child, the first of the australopithecines to be discovered, is the type specimen for Aust
The Taung Child, the first of the australopithecines to be discovered, is the type specimen for Aust
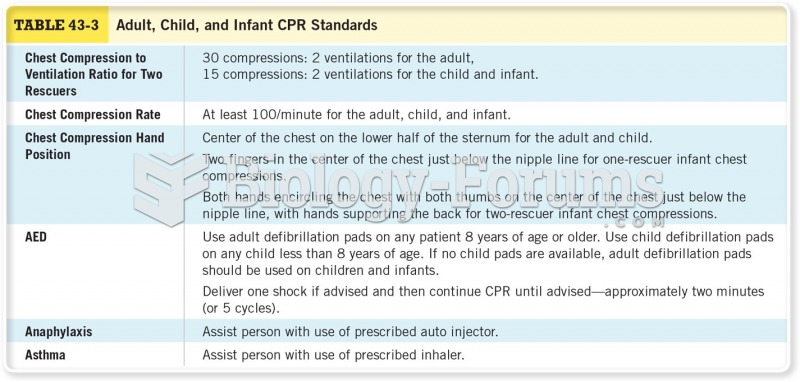 Adult, Child, and Infant CPR Standards Cont
Adult, Child, and Infant CPR Standards Cont
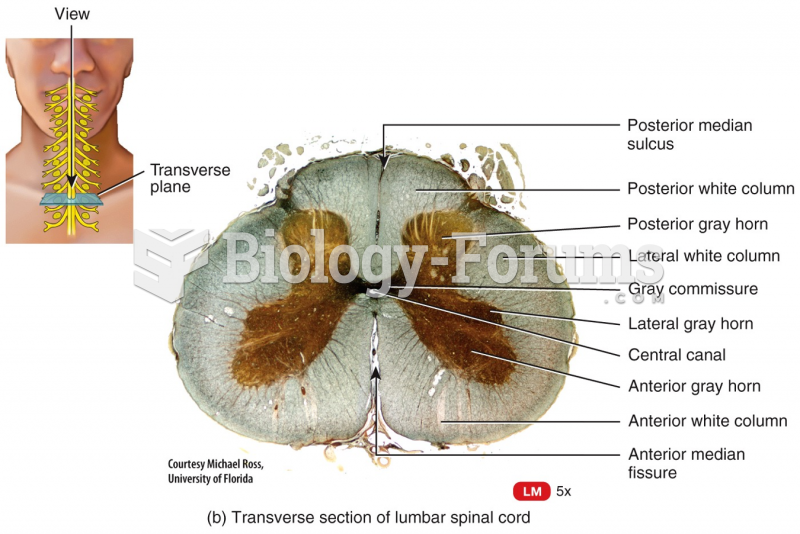 Internal Anatomy of the Spinal Cord
Internal Anatomy of the Spinal Cord