Answer to Question 1
ANS: A
A. Correct response: In a patient who has airflow obstruction, an important problem encountered with patient triggering is the inspiratory threshold load imposed by the auto-PEEP. Auto-PEEP must be overcome by the inspiratory muscles before airway pressure and flow change to produce a signal to the ventilator that a patient is attempting to trigger a breath. This condition is manifested by a patient who appears to be contracting the inspiratory muscles, but in whom the ventilator detects no inspiratory activity. If an esophageal balloon is unavailable, trial and error can be used to provide extrinsic (applied) PEEP to cause triggering. Clinically, the therapist can add 2 to 5 cm H2O, and observe the patient's response. If successful, the patient's effort to trigger the breaths should become less as the appropriate level of PEEP is provided. Increasing dyspnea and other signs of increasing intrathoracic pressure (e.g., increasing blood pressure, worsening signs of hyperinflation) suggest that excessive PEEP is being provided.
B. Incorrect response: See explanation A.
C. Incorrect response: See explanation A.
D. Incorrect response: In rare cases of severe airflow obstruction, heavy sedation and sometimes neuromuscular blocking agents may be required to remove any dyssynchrony that raises peak inspiratory pressures or inappropriately increases minute ventilation. In most cases, however, patient triggering is generally preferred to time triggering because it can help improve comfort and forestall ventilatory muscle atrophy.
Answer to Question 2
ANS: C
A. Correct response: Because alveolar inflammation, flooding, and collapse from airflow obstruction are not major features of acute respiratory failure from airflow obstruction, applying PEEP to maintain alveolar recruitment is generally unnecessary. Moreover, because applied PEEP can further overdistend obstructed regions, PEEP should probably be avoided unless clear regions of atelectasis or alveolar edema exist. Fio2 adjustments can be used to provide adequate oxygenation. Applied PEEP, however, may help the patient trigger breaths in the presence of high levels of auto-PEEP. The hypoxemia these patients experience results from simple V/Q abnormalities, manageable by changes in Fio2.
B. Incorrect response: See explanation A.
C. Incorrect response: See explanation A.
D. Incorrect response: See explanation A

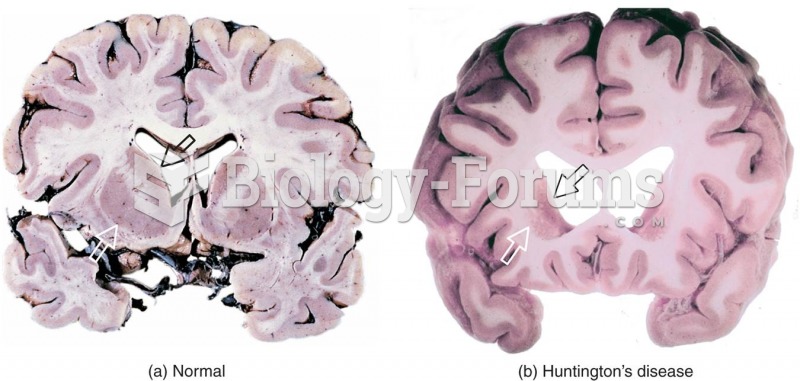 Huntington’s Disease
Huntington’s Disease
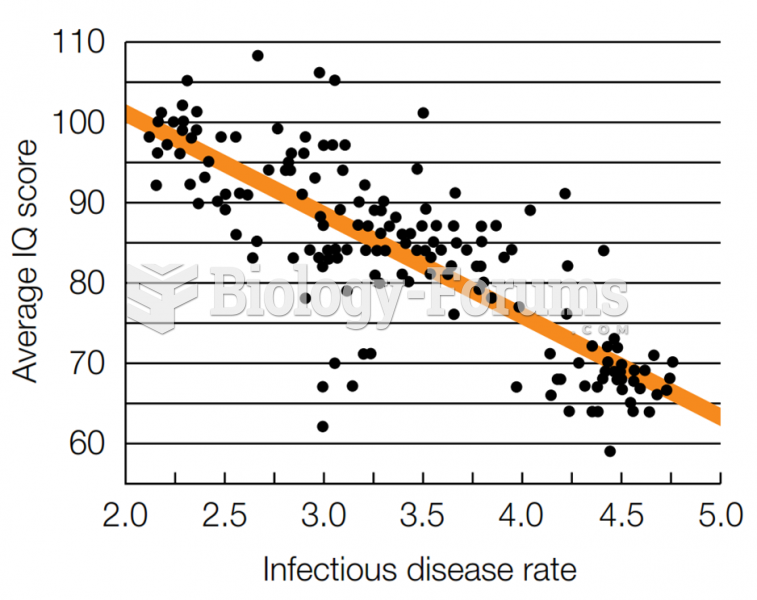 Inverse Relation Between IQ and Disease. Could this explain the Flynn effect?
Inverse Relation Between IQ and Disease. Could this explain the Flynn effect?
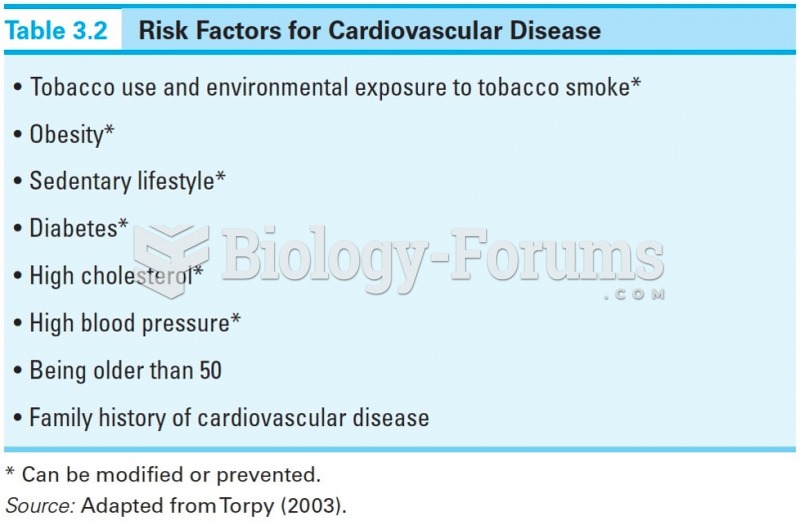 Risk Factors for Cardiovascular Disease
Risk Factors for Cardiovascular Disease
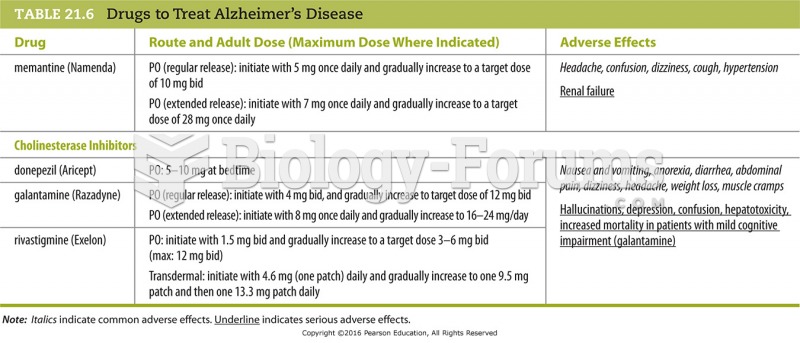 Drugs to Treat Alzheimer’s Disease
Drugs to Treat Alzheimer’s Disease
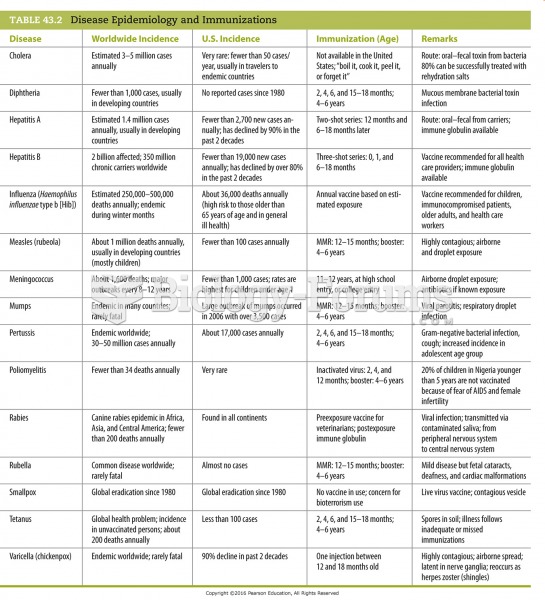 Disease Epidemiology and Immunizations
Disease Epidemiology and Immunizations
 Crown gall disease caused by Agrobacterium via plant transformation
Crown gall disease caused by Agrobacterium via plant transformation