A female patient who is 5'7 tall and weighs 68 kg is being mechanically ventilated with vol-ume-controlled continuous mandatory ventilation (VC-CMV), set rate 12,
patient trigger rate 25 breaths/min, tidal volume (VT) 500 mL, set flow rate 60 L/min, fractional inspired oxygen (FIO2) 40, positive end-expiratory pressure (PEEP) 5 cm H2O. The patient is currently in distress using accessory muscles of inspiration. The respiratory therapist performs a patient-ventilator system check. The flow-time waveform shows a failure of the expiratory flow to return to zero before the next breath is triggered. The most appropriate action for the respira-tory therapist to take includes which of the following?
a. Sedate the patient.
b. Switch to pressure-controlled continuous mandatory ventilation (PC-CMV).
c. Decrease set rate to 8 breaths/min.
d. Switch to volume-controlled intermittent mandatory ventilation (VC-IMV).
Question 2
A 6'2 male patient is being ventilated in the volume-controlled continuous mandatory ventilation (VC-CMV) mode with a set tidal volume (VT) of 650 mL. There is 40 mL of mechanical dead space. Calculate the final alveolar ventilation.
a. 432 mL
b. 445 mL
c. 510 mL
d. 535 mL

 Sika Deer Female
Sika Deer Female
 In the Tai Forest a female chimp demonstrates a skill once thought to be unique to humans. Here she
In the Tai Forest a female chimp demonstrates a skill once thought to be unique to humans. Here she
 A pacemaker in a patient’s chest.
A pacemaker in a patient’s chest.
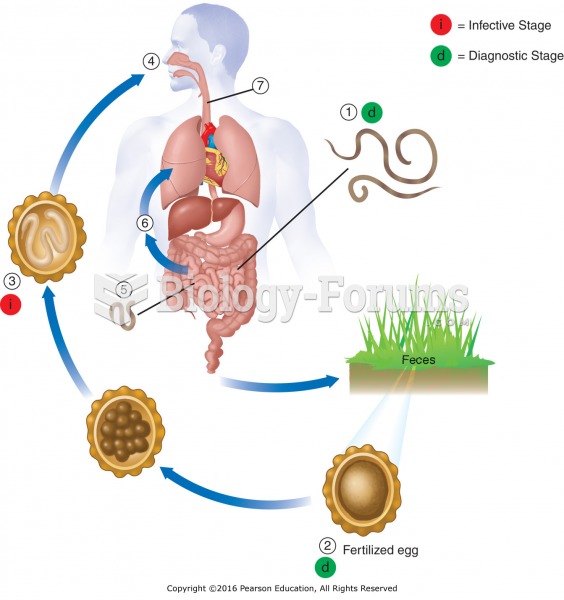 Life cycle of Ascaris: Adult worms (1) live in the lumen of the small intestine. A female may ...
Life cycle of Ascaris: Adult worms (1) live in the lumen of the small intestine. A female may ...
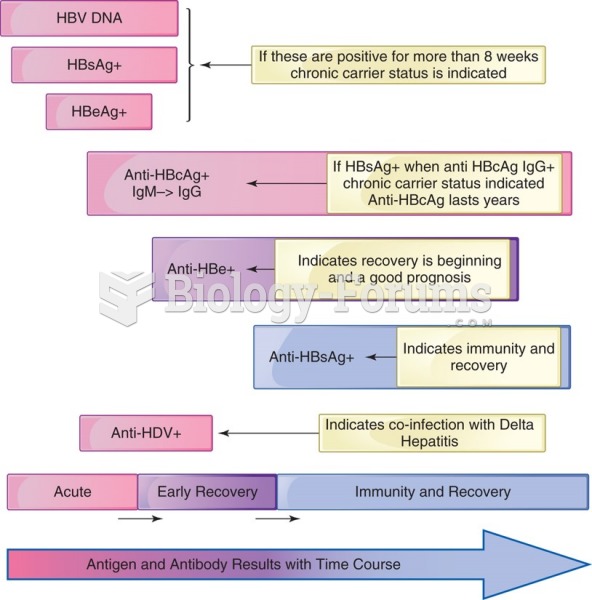 Hepatitis B antigens and antibody in an acutely infected patient with recovery. Note the indicators ...
Hepatitis B antigens and antibody in an acutely infected patient with recovery. Note the indicators ...
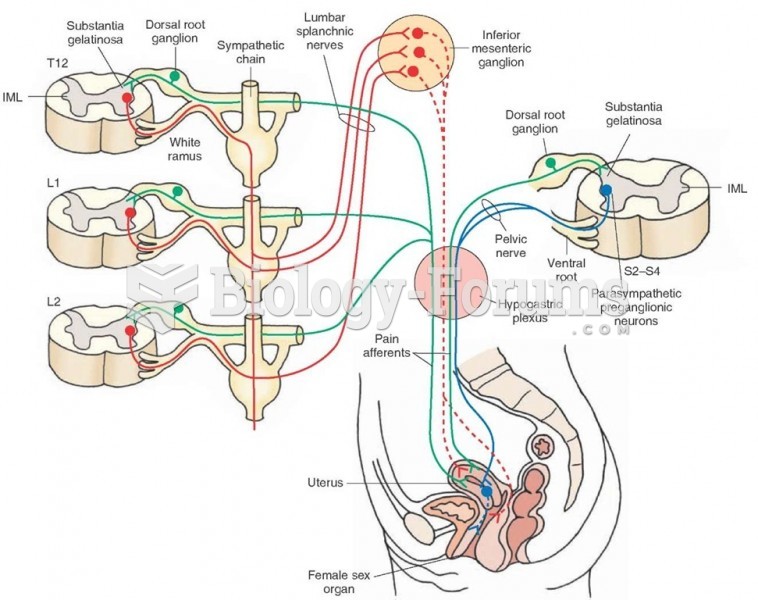 Autonomic innervation of the female reproductive system
Autonomic innervation of the female reproductive system