A client has been placed in seclusion. Which client behavior would have warranted this intervention?
1. The client is manic, has been flirtatious towards staff and refused morning medication, and has verbalized a plan to leave
2. The client is psychotic, sits in the corner with hands over ears, and displays increased suspiciousness of and agitation towards others despite recently receiving 1mg risperidone (Risperdal) PRN
3. The client is depressed and wants to be left alone to rest
4. The client is suicidal, has been banging head against the table in the day room, and was unresponsive to staff's verbal redirection
Question 2
A client with paranoid schizophrenia is experiencing visual hallucinations of people jumping out of nowhere. The client keeps striking the wall.
Repeated attempts by the nurse to orient the client to reality and reassure the client of safety have failed. What would be the nurse's next de-escalation approach? 1. Offer the client a PRN medication
2. Apply soft limb restraints on client's wrists
3. Have several staff demobilize the client so that forcible injection can be administered
4. Call security to assist in placing the client in seclusion

 A client is having an endoscopy performed by a physician who views the upper gastrointestinal intern
A client is having an endoscopy performed by a physician who views the upper gastrointestinal intern
 Sugar Cube-Sized Robotic Ants Mimic Real Foraging Behavior
Sugar Cube-Sized Robotic Ants Mimic Real Foraging Behavior
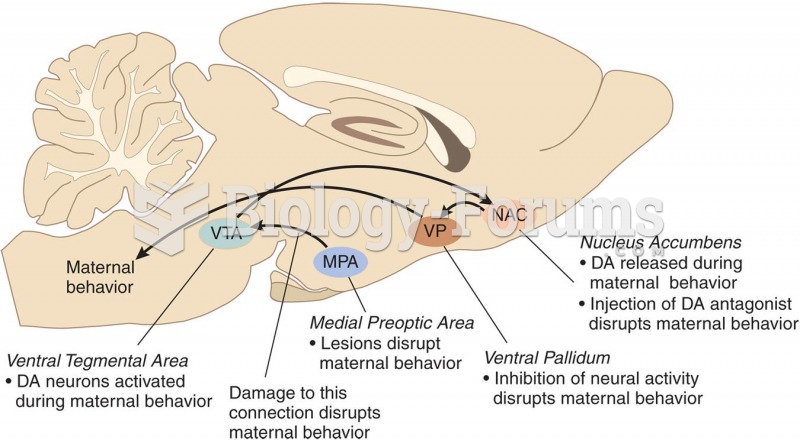 Neural Circuits and Maternal Behavior
Neural Circuits and Maternal Behavior
 Measuring the client’s blood pressure
Measuring the client’s blood pressure
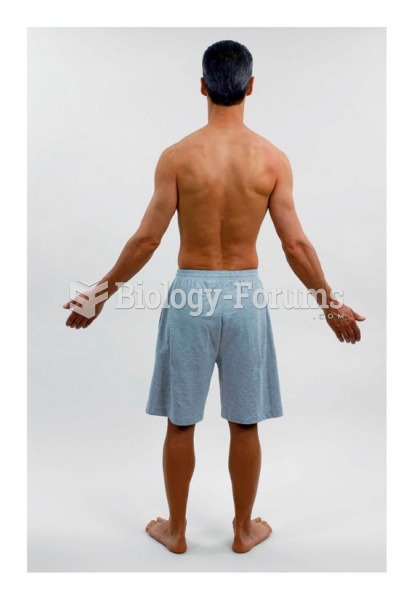 Survey and posture of client: Lateral view
Survey and posture of client: Lateral view
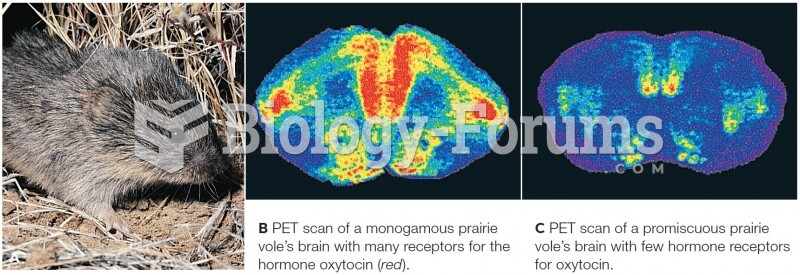 Studying the genetic roots of mating and bonding behavior
Studying the genetic roots of mating and bonding behavior