This topic contains a solution. Click here to go to the answer
|
|
|

 Pupil Assessment, Starting Position with Penlight to Side of Pupil
Pupil Assessment, Starting Position with Penlight to Side of Pupil
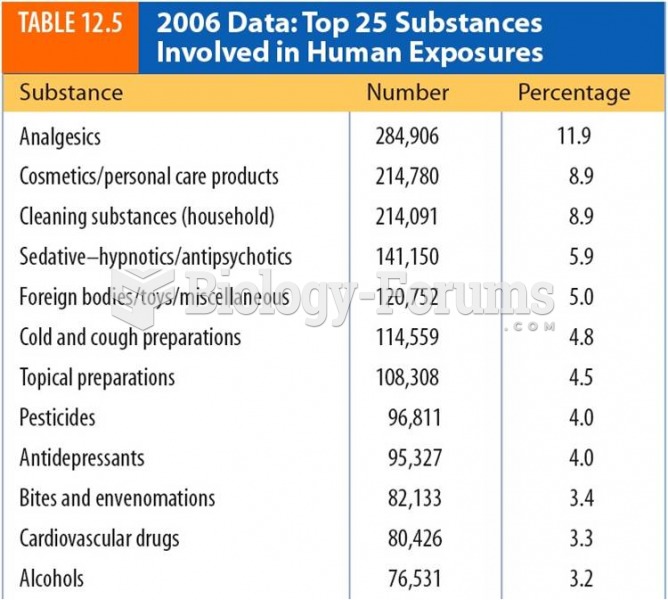 2006 Data:Top 25 Substances Involved in Human Exposures
2006 Data:Top 25 Substances Involved in Human Exposures
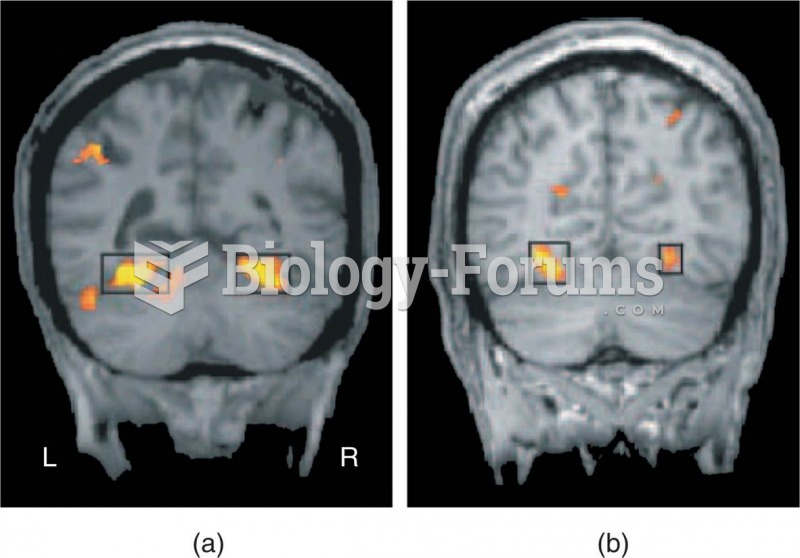 The Parahippocampal Place Area
The Parahippocampal Place Area
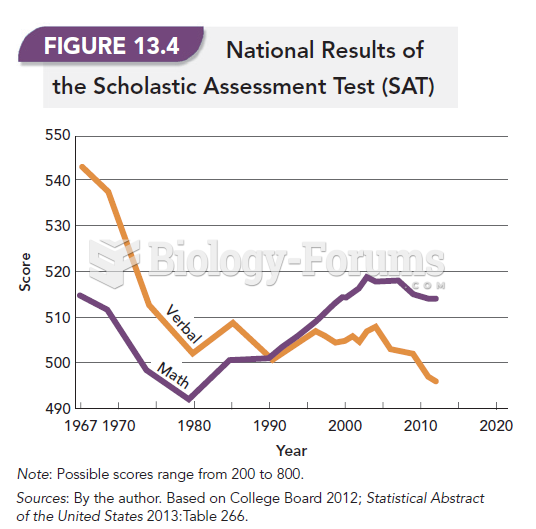 National Results of the Scholastic Assessment Test (SAT)
National Results of the Scholastic Assessment Test (SAT)
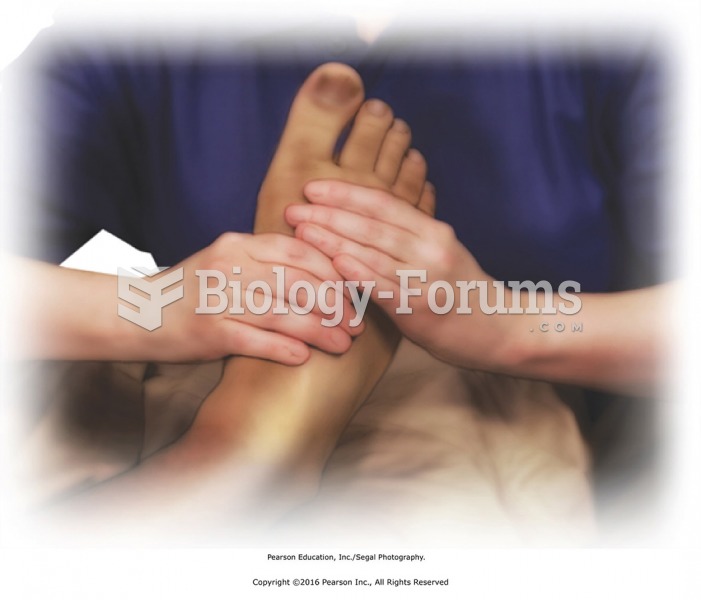 Squeeze the foot lightly from heel to toes. Fingers of hands on top with thumbs around the sides and ...
Squeeze the foot lightly from heel to toes. Fingers of hands on top with thumbs around the sides and ...
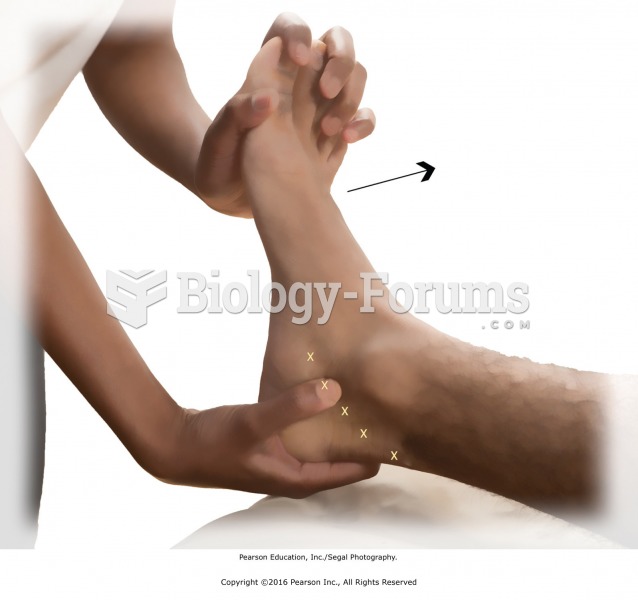 Inside ankle press. Place the heel of your left hand on the ball of the recipient’s right foot, ...
Inside ankle press. Place the heel of your left hand on the ball of the recipient’s right foot, ...