Answer to Question 1
Correct Answer: 2
Rationale 1: Restlessness is observable so it is not an example of subjective data.
Rationale 2: Subjective data can be described or verified only by that person and are apparent only to the person affected. Subjective data include the client's sensations, feelings, beliefs, attitudes, and perceptions of personal health status and life situations.
Rationale 3: Not being talkative is observable so it is not an example of subjective data.
Rationale 4: Paleness with diaphoresis iare observable so it is not an example of subjective data.
Answer to Question 2
Correct Answer: 1
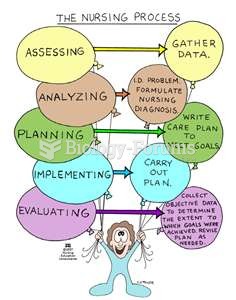
Rationale 1: Assessment is the collection, organization, validation, and documentation of data. Assessment is carried throughout the nursing process, as in this case. Even though performing the dressing change is implementation, noticing the new skin breakdown is assessment.
Rationale 2: Diagnosis is identifying the client's response to the problem. Implementation is what the nurse does to help the client reach a goal, and then the goal is evaluated.
Rationale 3: Even though performing the dressing change is implementation, noticing the new skin breakdown is assessment.
Rationale 4: The goal of the intervention is evaluated but that is not what is being described in this item..

 NUrse :0
NUrse :0
 To increase pressure using body weight, lean on your client.
To increase pressure using body weight, lean on your client.
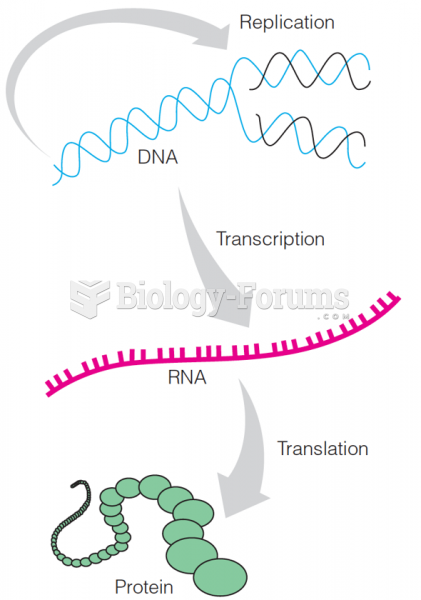 The flow of genetic information in a typical cell
The flow of genetic information in a typical cell
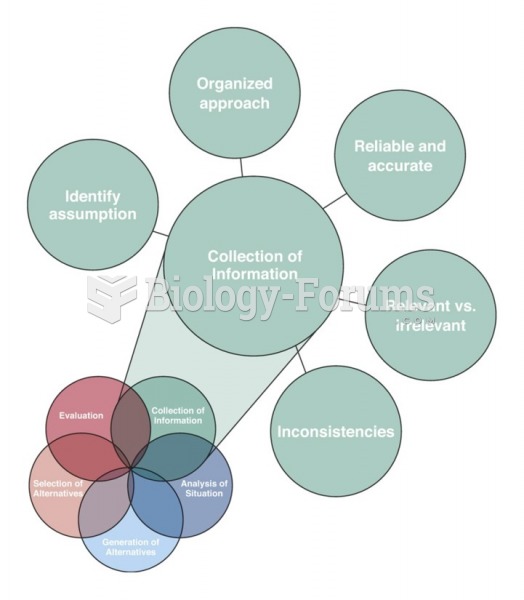 The five skills of the element Collection of Information
The five skills of the element Collection of Information
 Fluency with Information Technology: Skills, Concepts, and Capabilities
Fluency with Information Technology: Skills, Concepts, and Capabilities
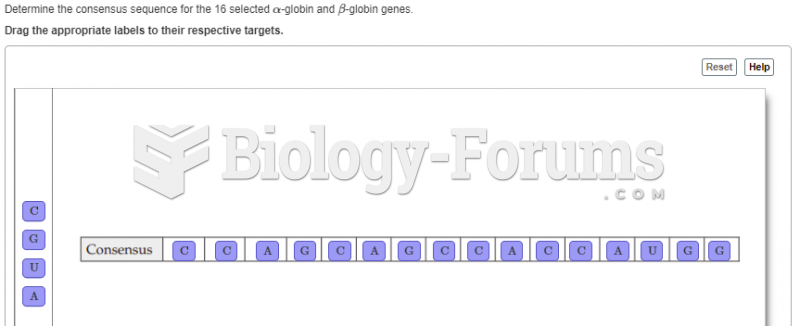 8.The following table contains DNA-sequence information compiled by Marilyn Kozak (1987). The ...
8.The following table contains DNA-sequence information compiled by Marilyn Kozak (1987). The ...