Answer to Question 1
ANS: B
Pain is a subjective experience and patients' pain experiences will not all be the same. The nurse needs to assess the patient's pain further. After assessing the patient's pain, if it is time for a dose of pain medication, the nurse should administer it. If the nurse's clinical judgment indicates an additional dose of medication is warranted, the provider can be contacted. The nurse should not dismiss the patient's pain by telling him/her that it is unreasonable.
Answer to Question 2
ANS: A
This patient has orthostatic hypotension, which is a drop of 20 mm Hg in systolic reading and 10 mm Hg in diastolic reading when the patient stands up from a sitting or lying position. The patient's cardiovascular system does not compensate for this, so the patient is at risk of becoming dizzy and fainting. The nurse instructs the patient to call for assistance before getting up to prevent a fall. The nurse should document the findings but needs to do more. These findings are not normal, so the nurse should not tell the patient that they are. The patient may need to be assessed sooner than 1 hour.

 Checking teeth and other physical examinations are an important part of horse care.
Checking teeth and other physical examinations are an important part of horse care.
 Critical thinking involves analysis in which the nurse examines patient data available from a variet
Critical thinking involves analysis in which the nurse examines patient data available from a variet
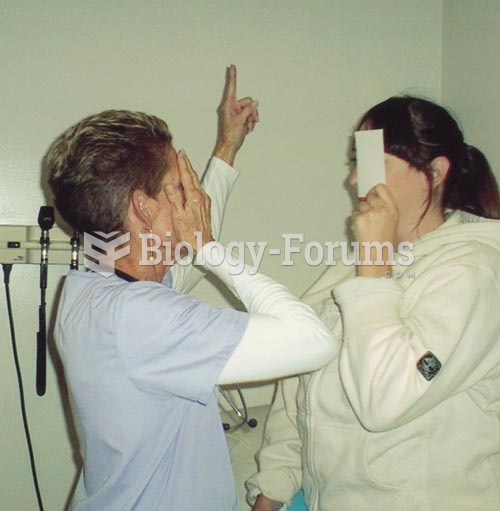 Testing Visual Fields by Confrontation: The nurse and patient should be approximately at an eye to e
Testing Visual Fields by Confrontation: The nurse and patient should be approximately at an eye to e
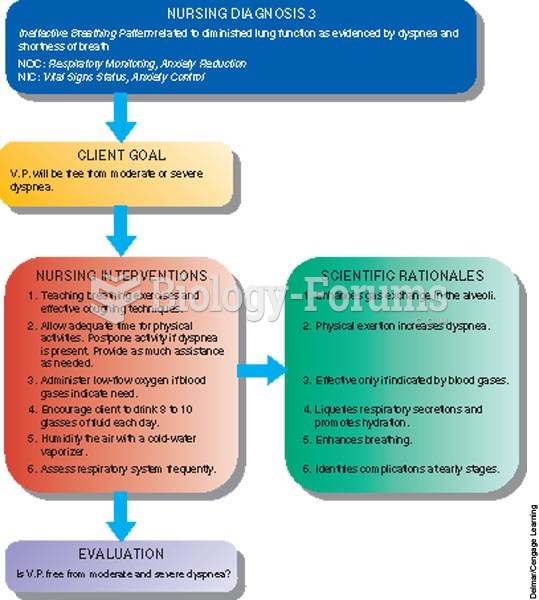 Concept Care Map
Concept Care Map
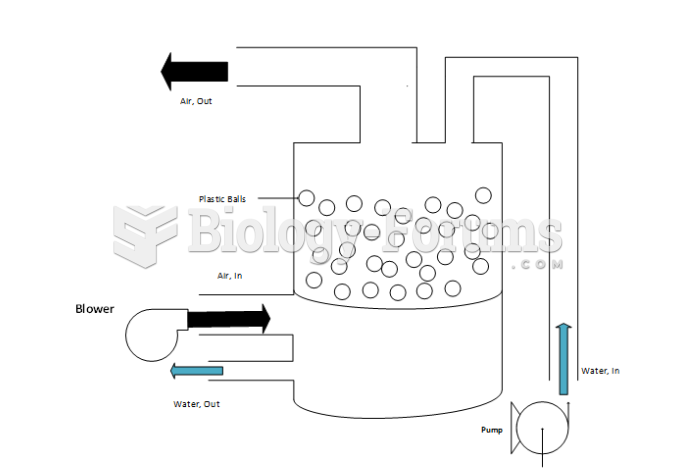 Schematic Diagram of the fluidized bed for the experiment (CHE415 Unit Operations)
Schematic Diagram of the fluidized bed for the experiment (CHE415 Unit Operations)
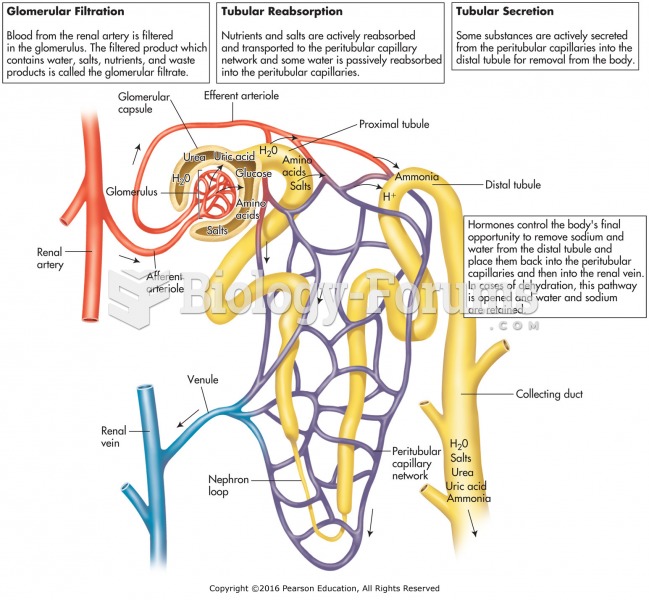 A functional renal unit.
A functional renal unit.