Answer to Question 1
ANS: C
The current regimen of choice for patients taking highly emetogenic drugs consists of three agents: aprepitant plus dexamethasone plus a 5-HT3 antagonist, such as ondansetron. Aprepitant has a prolonged duration of action and can prevent delayed CINV as well as acute CINV. Increasing the dose of ondansetron will not help treat the delayed CINV. Glucocorticoids should be given intermittently and for short periods to avoid side effects. Changing the ondansetron to aprepitant is not recommended.
Answer to Question 2
ANS: C
If IV administration must be done with this drug, it should be given through a large-bore, freely flowing line. The site should be monitored closely for local burning or pain or any sign of extravasation, which can cause abscess formation, tissue necrosis, and gangrene requiring amputation. Giving the medication as a rapid IV push or through microbore tubing does not adequately slow the infusion or dilute the drug. Dry mouth and sedation are expected side effects of this drug and are not dangerous.

 The patient interview often requires note taking.
The patient interview often requires note taking.
 Patient Position for Posterior Percussion
Patient Position for Posterior Percussion
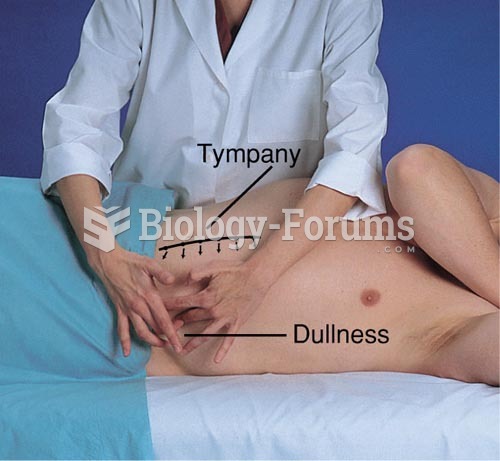 Percussion for Ascites: Shifting Dullness, Patient on Left Side
Percussion for Ascites: Shifting Dullness, Patient on Left Side
 What a tremendous photo for sociologists! Seldom are we treated to such cultural contrasts. Can you ...
What a tremendous photo for sociologists! Seldom are we treated to such cultural contrasts. Can you ...
 Each patient is greeted by the receptionist.
Each patient is greeted by the receptionist.
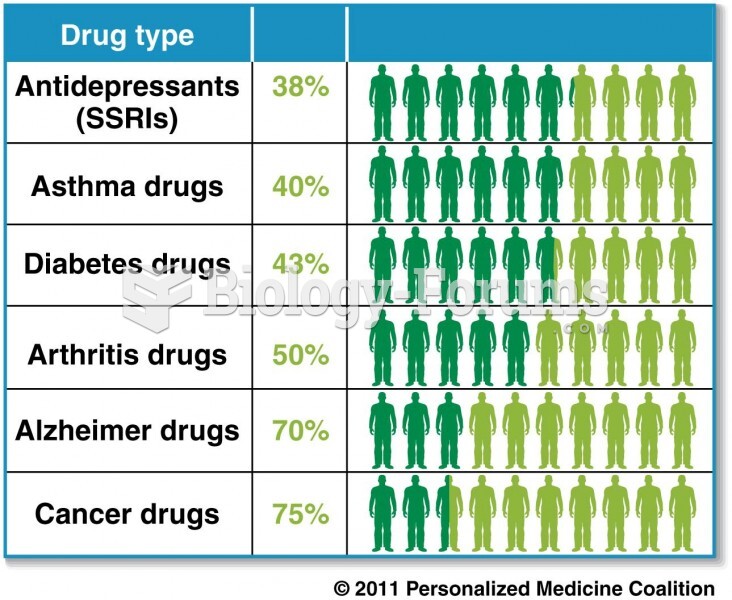 Variations in patient response to drugs
Variations in patient response to drugs