This topic contains a solution. Click here to go to the answer
|
|
|

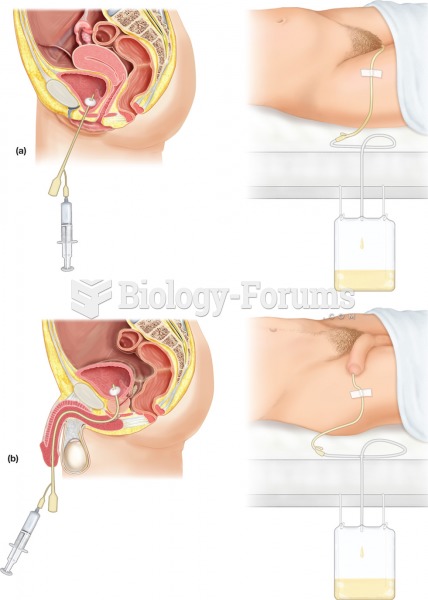 Urinary catheterization. The procedure involves the insertion of a flexible tube, or catheter, throu
Urinary catheterization. The procedure involves the insertion of a flexible tube, or catheter, throu
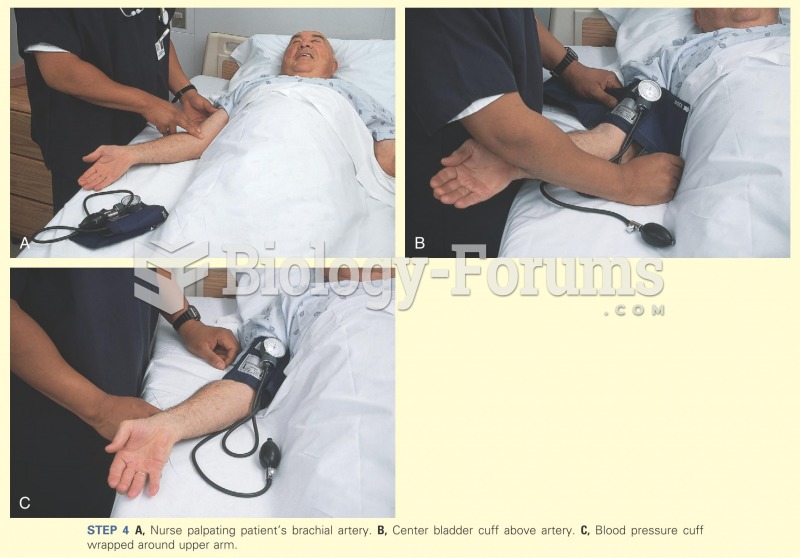 Nurse palpating the patient's brachial artery
Nurse palpating the patient's brachial artery
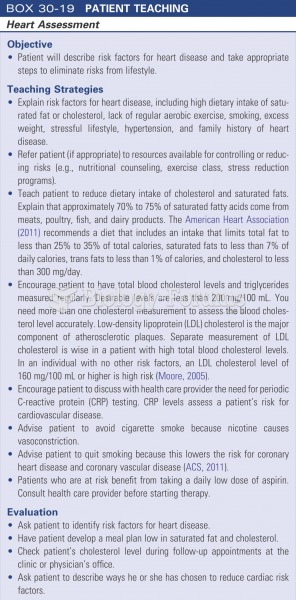 Patient teaching: heart assessment
Patient teaching: heart assessment
 A surgeon holds a pacemaker next to an X-ray of a pacemaker implanted in a patient’s chest.
A surgeon holds a pacemaker next to an X-ray of a pacemaker implanted in a patient’s chest.
 Patient with DiGeorge syndrome. Note low set ears and wide set downward slanting eyes; often these ...
Patient with DiGeorge syndrome. Note low set ears and wide set downward slanting eyes; often these ...
 National Patient Safety Goals for Acute-Care Hospitals
National Patient Safety Goals for Acute-Care Hospitals