Answer to Question 1
There are several drawbacks to medical treatments for insomnia. First, benzodiazepine medications can cause excessive sleepiness. Second, people can easily become dependent on them and rather easily misuse them, deliberately or not. Third, these medications are meant for short-term treatment and are not recommended for use longer than four weeks. Longer use can cause dependence and rebound insomnia. A newer concern for some medications (e.g., Ambien) is that they may increase the likelihood of sleepwalking-related problems, such as sleep-related eating disorder. Therefore, although medications may be helpful for sleep problems that will correct themselves in a short period (e.g., insomnia because of anxiety related to hospitalization), they are not intended for long-term chronic problems.
Answer to Question 2
In anorexia nervosa, the most important initial goal is to restore the patient's weight to a point that is at least within the low-normal range (American Psychiatric Association, 2010). If body weight is below 85 percent of the average healthy body weight for a given individual, or if weight has been lost rapidly and the individual continues to refuse food, inpatient treatment is recommended (American Psychiatric Association, 2010; Casper, 1982) because severe medical complications, particularly acute cardiac failure, could occur if weight is not restored immediately. If the weight loss has been more gradual and seems to have stabilized, weight restoration can be accomplished on an outpatient basis.
Restoring weight is probably the easiest part of treatment. Clinicians who treat patients in different settings, as reported in a variety of studies, find that at least 85 percent will be able to gain weight. The gain is often as much as a half pound to a pound a day until weight is within the normal range. Knowing they can leave the hospital when their weight gain is adequate is often sufficient to motivate individuals with anorexia nervosa. Julie gained about 18 pounds during her five-week hospital stay.
Without attention to the patient's underlying dysfunctional attitudes about body shape, as well as interpersonal disruptions in her life, she will almost always relapse. For restricting anorexics, the focus of treatment must shift to their marked anxiety over becoming obese and losing control of eating, as well as to their undue emphasis on thinness as a determinant of self-worth, happiness, and success. In this regard, effective treatments for restricting anorexics are similar to those for patients with bulimia nervosa. Extended (one-year) outpatient CBT was found to be significantly better than continued nutritional counseling in preventing relapse after weight restoration, with only 22 percent failing (relapsing or dropping out) with CBT versus 73 percent failing with nutritional counseling. In addition, every effort is made to include the family to accomplish two goals. First, the negative and dysfunctional communication in the family regarding food and eating must be eliminated, and meals must be made more structured and reinforcing. Second, attitudes toward body shape and image distortion are discussed at some length in family sessions. Unless the therapist attends to these attitudes, individuals with anorexia nervosa are likely to face a lifetime preoccupation with weight and body shape, struggle to maintain marginal weight and social adjustment, and be subject to repeated hospitalization. Family therapy directed at the goals mentioned above seems effective, particularly with young girls (less than 19 years of age) with a short history of the disorder

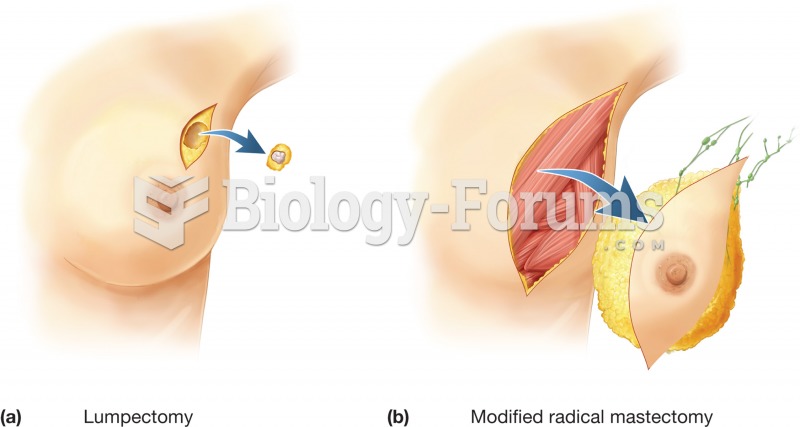 Breast surgery. Surgical removal of all or part of the breast is a treatment against the spread of b
Breast surgery. Surgical removal of all or part of the breast is a treatment against the spread of b
 Municipal Water Treatment Plant
Municipal Water Treatment Plant
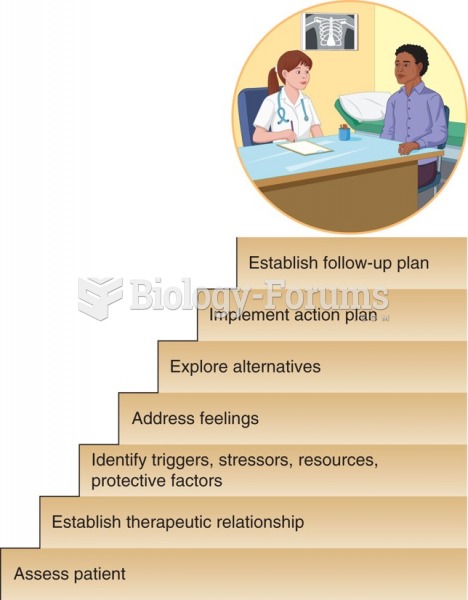 Roberts's Assessment, Crisis Intervention, and Trauma Treatment (ACT) model.
Roberts's Assessment, Crisis Intervention, and Trauma Treatment (ACT) model.
 How to solve word problems with two unknowns (Question 1)
How to solve word problems with two unknowns (Question 1)
 Social Problems: A Critical Power-Conflict Perspective
Social Problems: A Critical Power-Conflict Perspective
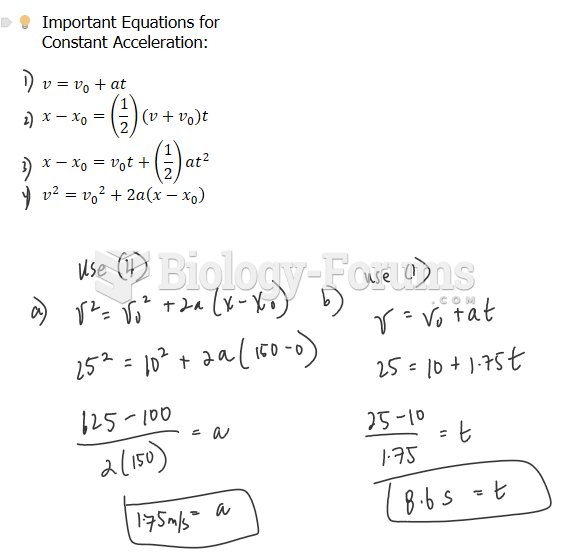 Physics - Motion (Please help me solve these problems, I really need help)
Physics - Motion (Please help me solve these problems, I really need help)