Answer to Question 1
Young people who suffer from persistent depressive disorder (PDD) experience symptoms of depressed mood that occur for most of the day, on most days, and persist for at least 1 year. They are unhappy or irritable most of the time. (The sad and gloomy life of Eeyore the donkey in the 100 Acre Wood likely qualifies for a diagnosis of PDD.) Combined with their chronic depressed (or irritable) mood, these children also display at least two somatic (e.g., eating problems, sleep disturbances, low energy) or cognitive symptoms (e.g., lack of concentration, low self-esteem, feelings of hopelessness) that are present while they are depressed. Although the symptoms of PDD are chronic, they are less severe than those for children with MDD. PDD is a new category in DSM-5; it combines the previous DSM-IV categories of Dysthymic Disorder and MDDChronic. This was done because of the lack of differences between youths with a dysthymic disorder and those with a chronic type of major depression. In comparison to nonchronic MDD, chronic forms of depression, whether referred to as dysthymic disorder, chronic major depression, or PDD are associated with a poorer response to treatment, greater long-term morbidity at follow-up, and greater familial loading for affective disorders (McCullough et al., 2003).
Answer to Question 2
The modest increase in depression from preschool to elementary school is likely not biologically based, but rather is a reflection of the school-age child's growing self-awareness and cognitive capacity, verbal ability to report symptoms, and increased performance and social pressures. In contrast, the sharp increase in depression in adolescence appears to be the result of biological maturation at puberty interacting with important developmental changes that occur during this tumultuous period. This hypothesis is supported by the emergence of large sex differences in depression after puberty, the emergence of bipolar disorder, and the relative stability in rates of depression through adolescence (Birmaher et al., 1996).

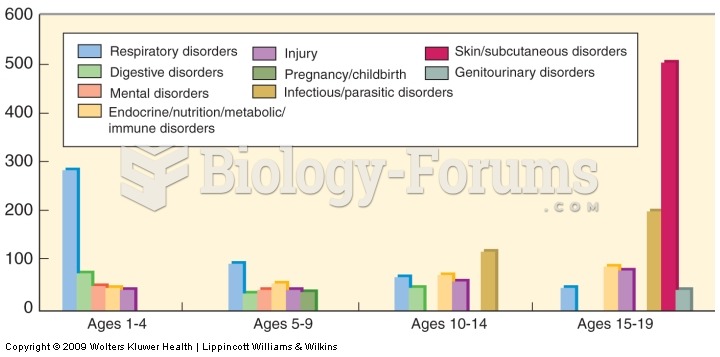 Major causes of hospitalization
Major causes of hospitalization
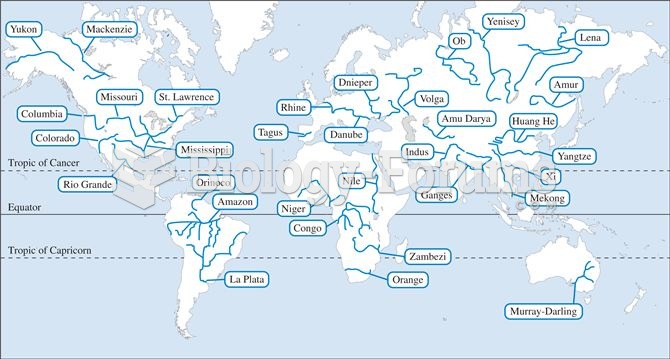 Major rivers throughout the world.
Major rivers throughout the world.
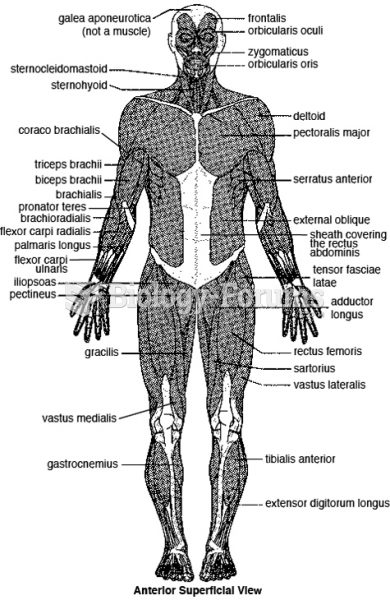 The major skeletal muscles—anterior superficial view.
The major skeletal muscles—anterior superficial view.
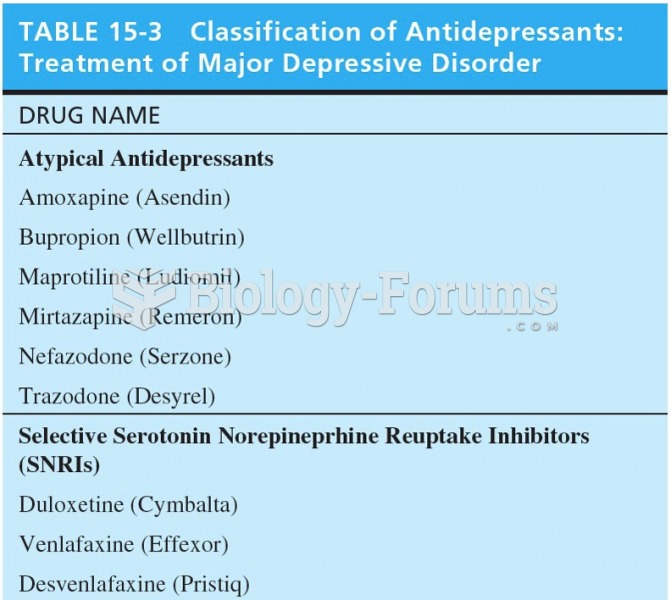 Classification of Antidepressants: Treatment of Major Depressive Disorder
Classification of Antidepressants: Treatment of Major Depressive Disorder
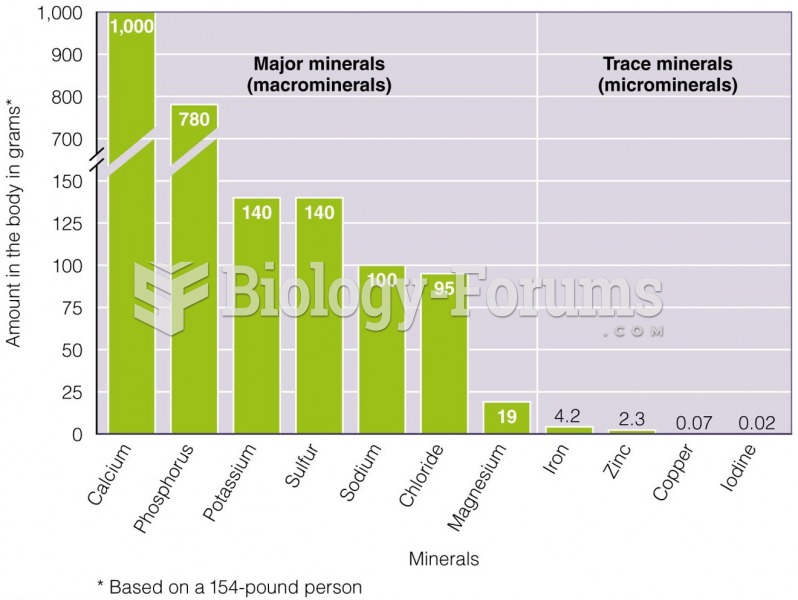 The Amounts of the Different Minerals in Your Body The major minerals are present in larger amounts
The Amounts of the Different Minerals in Your Body The major minerals are present in larger amounts
 Major phenotypic differences between maize and teosinte
Major phenotypic differences between maize and teosinte