A 36-year-old female patient with a history of asthma is admitted to the ICU from the emergen-cy department. Her respirations are 30, very labored, with accessory muscle use and bilateral in-spiratory and expiratory wheezing.
There is bilateral hyperresonance during chest percussion. A blood gas taken in the ICU after 1 hour of continuous aerosolized albuterol (15 mg) reveals: pH 7.38, partial pressure of carbon di-oxide (PaCO2) 42 mm Hg, partial pressure of oxygen (PaO2) 53 mm Hg, oxygen saturation (SaO2) 88, bicarbonate (HCO3) 25 mEq/L with nasal cannula 6 L/min. The patient is 5'5 and weighs 135 lb. The most appropriate action at this time is which of the following?
a. Continue current therapy with 20 mg al-buterol and reassess in 1 hour.
b. Noninvasive positive pressure ventilation (NPPV) with bilevel positive airway pres-sure (bilevel PAP), f = 12, inspiratory pos-itive airway pressure (IPAP) 28 cm H2O, expiratory positive airway pressure (EPAP) 3 cm H2O, fractional inspired ox-ygen (FIO2) 0.30
c. Intubate, use pressure-controlled continu-ous mandatory ventilation (PC-CMV), f = 8, peak inspiratory pressure (PIP) 28 cm H2O, TI 0.75 seconds, positive end-expiratory pressure (PEEP) 3 cm H2O, FIO2 1.0
d. Intubate, use volume-controlled continu-ous mandatory ventilation (VC-CMV), f = 12, tidal volume (VT) 600 mL, PF 40 L/min, PEEP 5 cm H2O, FIO2 0.60
Question 2
During mechanical ventilation, a patient with a closed head injury develops the Cushing re-sponse. This may be immediately managed by using which of the following?
a. Pressure-controlled continuous mandatory ventilation (PC-CMV) with positive end- expiratory pressure (PEEP)
b. Sedation and paralysis
c. Permissive hypercapnia
d. Iatrogenic hyperventilation

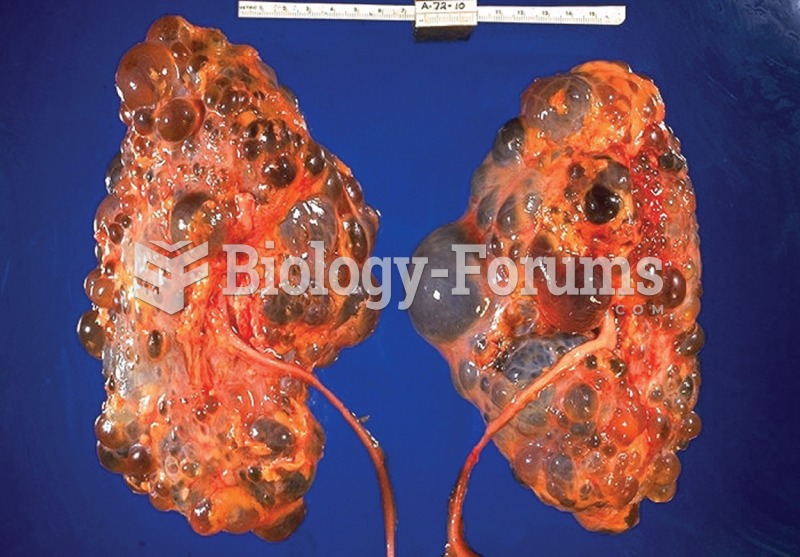 Polycystic kidney disease. Notice the presence of numerous fluid-filled sacs, or cysts, in these kid
Polycystic kidney disease. Notice the presence of numerous fluid-filled sacs, or cysts, in these kid
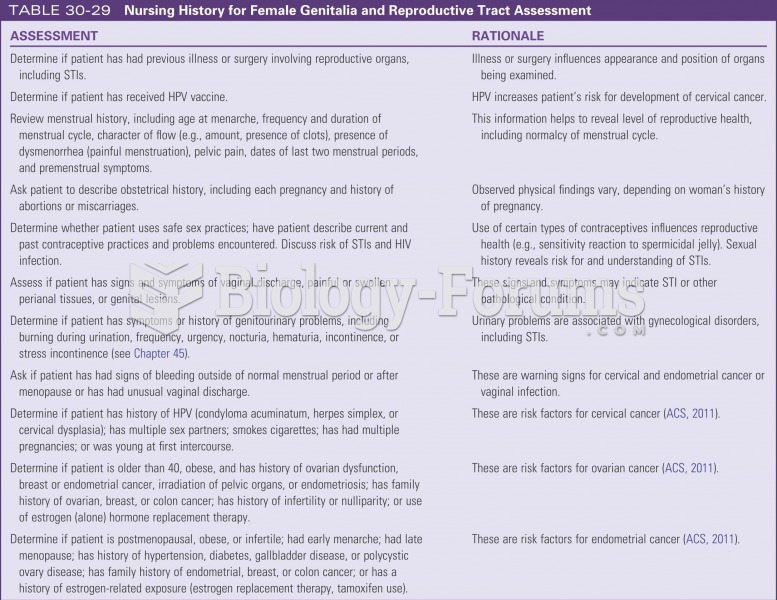 Nursing history for female genetalia and reproductive tract assessment
Nursing history for female genetalia and reproductive tract assessment
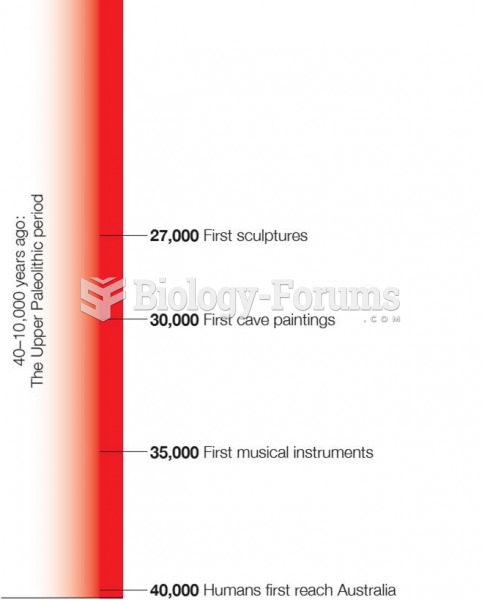 Time Line of Human History From Upper Paleolithic Period to the Present
Time Line of Human History From Upper Paleolithic Period to the Present
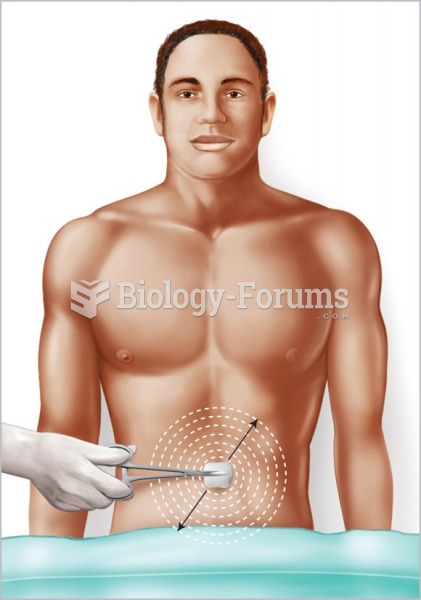 Preparing the Patient’s Skin for Surgical Procedures
Preparing the Patient’s Skin for Surgical Procedures
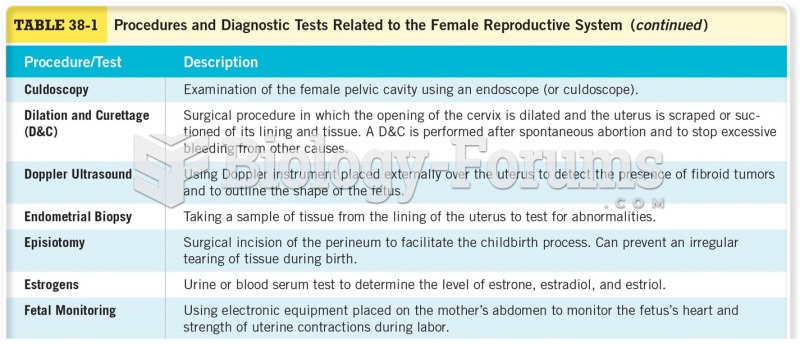 Procedures and Diagnostic Tests Related to the Female Reproductive System
Procedures and Diagnostic Tests Related to the Female Reproductive System
 Nitin earns $48,000 per year. Determine his gross earnings for each pay period if he is paid ...
Nitin earns $48,000 per year. Determine his gross earnings for each pay period if he is paid ...