Answer to Question 1
ANS: C
Myasthenia can occur at any age and may be associated with other autoimmune diseases. Limb weakness and fatigability of the affected muscles is a diagnostic sign. Symptoms are due to a variable blocking of neuromuscular transmission by autoantibodies that bind to acetylcholine receptors. Ocular, facial, masticatory, and pharyngeal muscles are most often affected. The eye symptoms of diplopia and ptosis are common early signs. Other symptoms include dysphagia, weakness in the extremities, and respiratory difficulties. Symptoms fluctuate during the day and the symptoms often relapse or remit over long periods of time, but ultimately the disease is progressive. Sustained activity of the affected muscles increases the weakness, and symptoms will improve with rest. Patients may require life support if respiratory effort is significantly affected.
Answer to Question 2
ANS: C
The signs and symptoms vary according to the underlying problem, but common symptoms include weight loss, flatulence, abdominal bloating, edema in the lower extremities resulting from protein deficiency, muscle weakness, possibly diarrhea or steatorrhea, dehydration, glossitis, and bruising. A variety of abnormal findings can be associated with malabsorption syndromes, including iron, folic acid, or B12 deficiency anemia; calcium deficiency; vitamins A, B, C, and D deficiencies; and niacin deficiency. A combination of weight loss, diarrhea, and anemia should raise the possibility of malabsorption. A variety of abnormal findings can be associated with malabsorption syndromes, including iron, folic acid, or B12 deficiency anemia; calcium deficiency; vitamins A, B, C, and D deficiencies; and niacin deficiency. There are as many diagnostics as there are causes of malabsorption. Measurement of fat in the stool is the most valuable diagnostic for diagnosing malabsorption, and a 3- to 4-day stool collection is advised. Stool specimens for ova, parasites and culture, and sensitivity will help to rule out infectious causes. Absorption tests, flat plate of the abdomen, upper GI with small bowel follow-through, endoscopy, and small bowel biopsy may be necessary for definitive diagnosis.

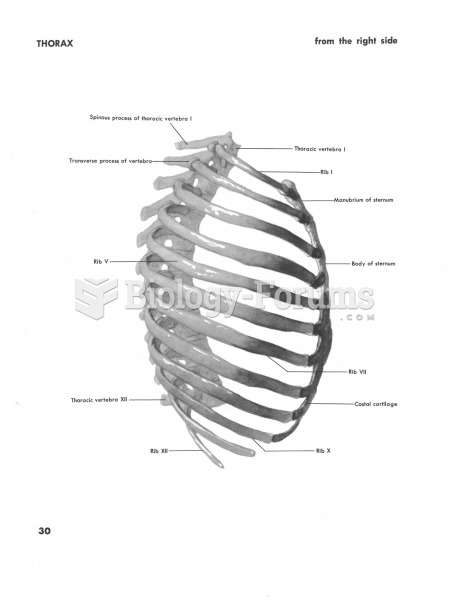 Thorax side
Thorax side
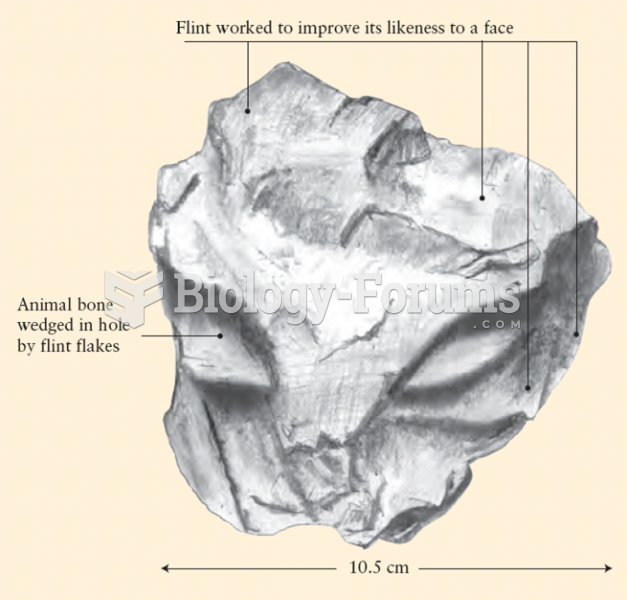 Neanderthal Expressive Culture: “Face” in Worked Flint
Neanderthal Expressive Culture: “Face” in Worked Flint
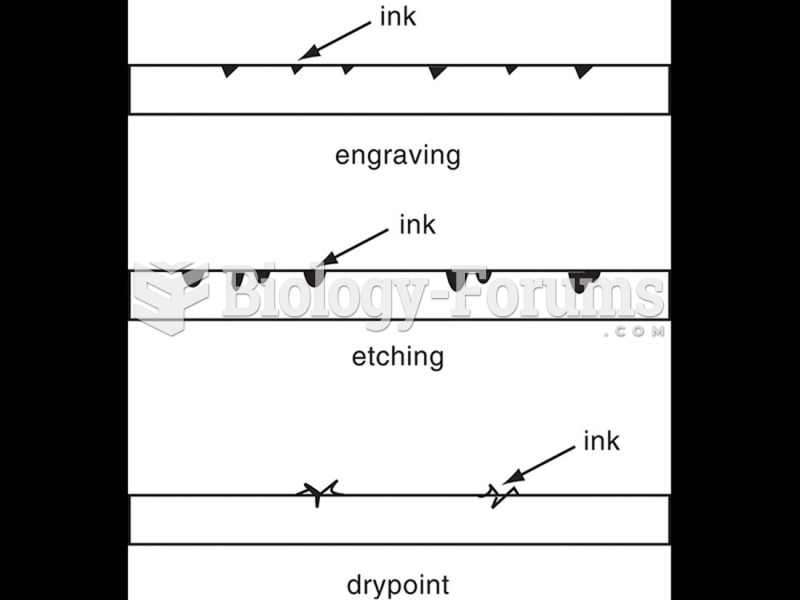 Intaglio printmaking techniques, side views.
Intaglio printmaking techniques, side views.
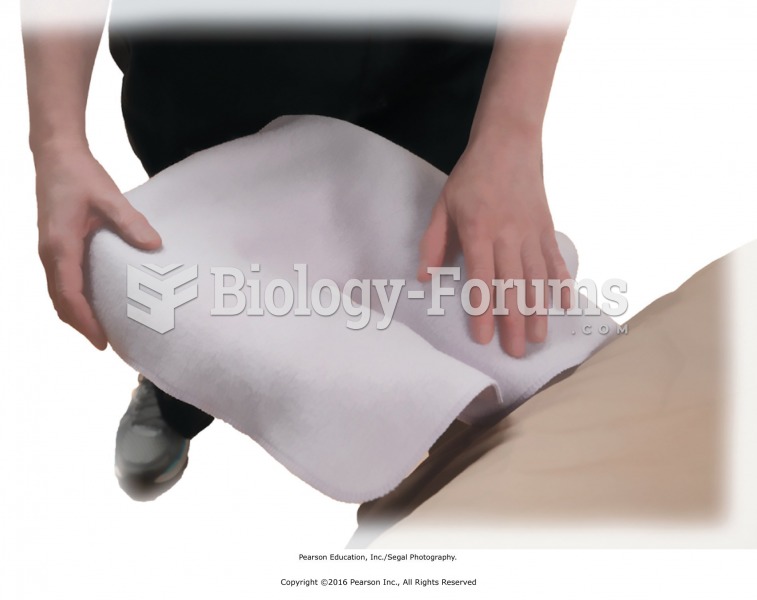 Use face cradle covers to prevent the client’s skin from touching the face cradle upholstery.
Use face cradle covers to prevent the client’s skin from touching the face cradle upholstery.
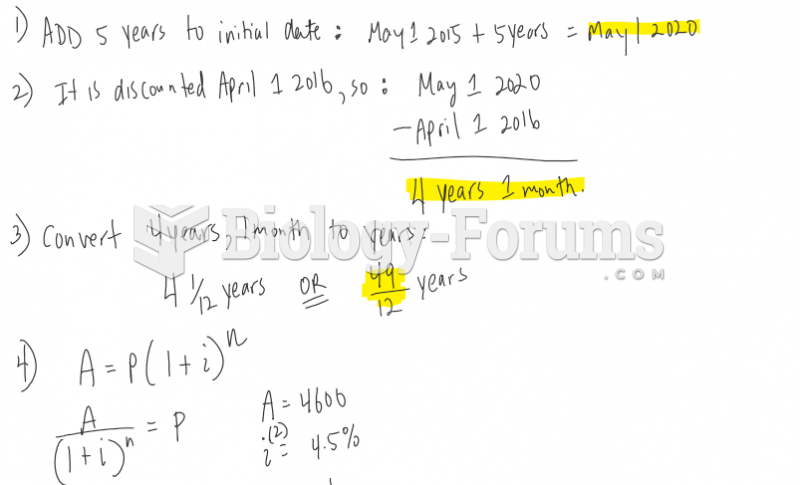 A non-interest-bearing five-year note for $54600.00 issued May 1, 2015, is discounted April 1, ...
A non-interest-bearing five-year note for $54600.00 issued May 1, 2015, is discounted April 1, ...