Answer to Question 1
ANS: B
Polymyalgia rheumatica is usually identified in adults aged 60 or older. The actual etiology of this condition is unknown. Giant cell arteritis occurs in about 15 of those with polymyalgia rheumatica, and the two conditions may be different expressions of the same etiology. The patient typically complains of sudden onset of widespread pain. Commonly affected sites include the neck, shoulders, and pelvis. Pain is accompanied by fatigue and stiffness. The stiffness is most profound in the morning. There is no actual muscle weakness. Unlike RA, there is no small joint inflammation and effusion.
Answer to Question 2
ANS: A
The anterior, medial, and lateral knee ligaments are vulnerable to injury in athletic activities. The mechanism through which the anterior cruciate ligament (ACL) is typically injured involves deceleration combined with sudden turning or pivoting. The medial collateral ligament (MCL) is most prone to injury through motions that place valgus stress on the knee. Compared with ACL and MCL injury, damage to the lateral collateral ligament (LCL) is much rarer but typically occurs when sudden varus stress is placed on the knee. The patient often relates history of an acute trauma followed by the onset of pain, swelling, and limited mobility. Often patients recall hearing or feeling a pop at the moment of injury and/or give-away sense. ACL injury is identified through a positive drawer (Fig. 14.9) and/or Lachman's test (Fig. 14.10). Laxity of the LCL is assessed by placing varus stress on the knee with the leg both extended and flexed.

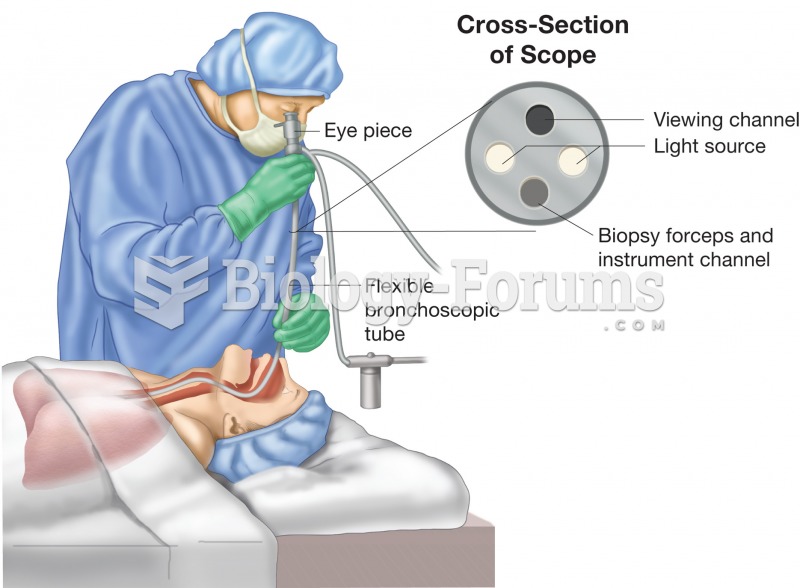 Bronchoscopy. Figure illustrates physician using a bronchoscope to inspect the patient’s bronchial t
Bronchoscopy. Figure illustrates physician using a bronchoscope to inspect the patient’s bronchial t
 Defibrillator. Defibrillators are devices that supply a voltage charge to the heart in the hope of r
Defibrillator. Defibrillators are devices that supply a voltage charge to the heart in the hope of r
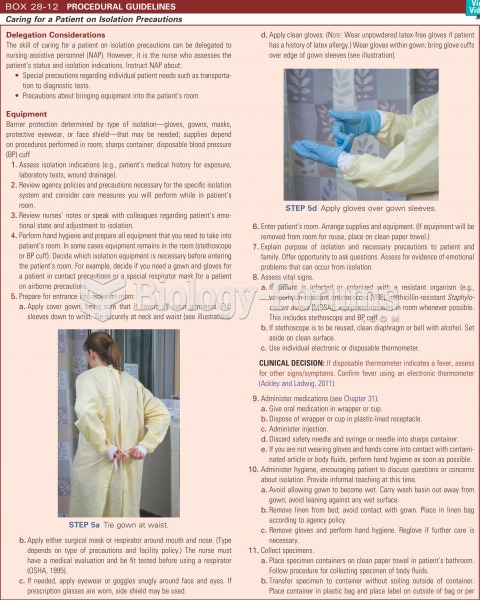 Caring for a patient on isolation precautions
Caring for a patient on isolation precautions
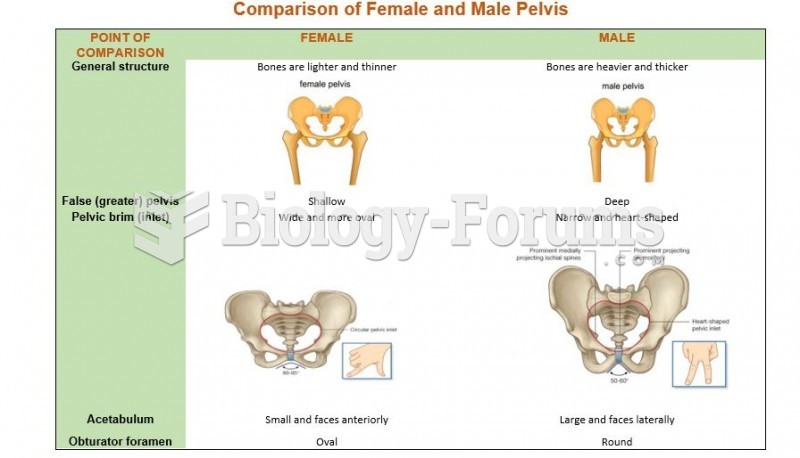 Comparison of Female and Male Pelvis
Comparison of Female and Male Pelvis
 Caucasoid Female
Caucasoid Female
 Random X inactivation in female placental mammals
Random X inactivation in female placental mammals