Answer to Question 1
2
Explanation:
1. The medication must be continued for life.
2. The parents should be cautioned to dress the child appropriately to prevent hypothermia.
3. The infant formula is not contraindicated with the prescribed medication.
4. The child will continue to need monitoring and intervention even if growth and development are not affected.
Answer to Question 2
2
Explanation:
1. Although this nursing diagnosis is applicable, pain is a lower priority than is risk for fluid volume deficit.
2. Adequate fluid volume is a critical physiologic need; therefore, this is the highest-priority nursing diagnosis.
3. Although this nursing diagnosis may be applicable, family coping is a lower priority than is risk for fluid volume deficit.
4. Although this nursing diagnosis may be applicable, a knowledge deficit is a psychosocial issue, and therefore a lower priority than is the physiologic need for adequate fluid volume.

 Many hobbies and leisure activities have some risk of health-related injuries
Many hobbies and leisure activities have some risk of health-related injuries
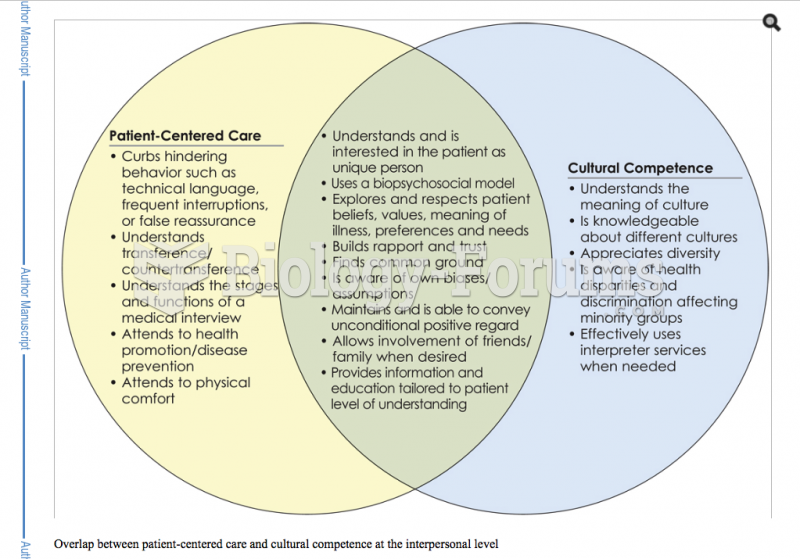 Health care - patient-centered
Health care - patient-centered
 When the United States gets stuck over a controversial issue—usually something a divided Congress ca
When the United States gets stuck over a controversial issue—usually something a divided Congress ca
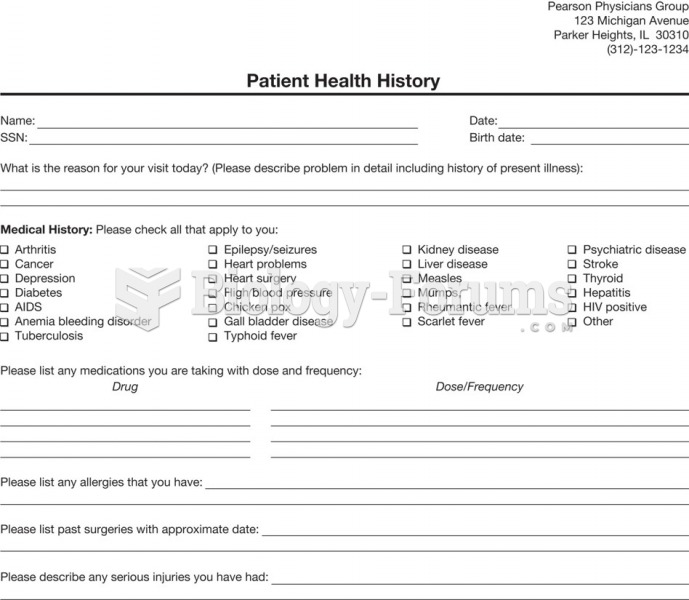 Patient health history form.
Patient health history form.
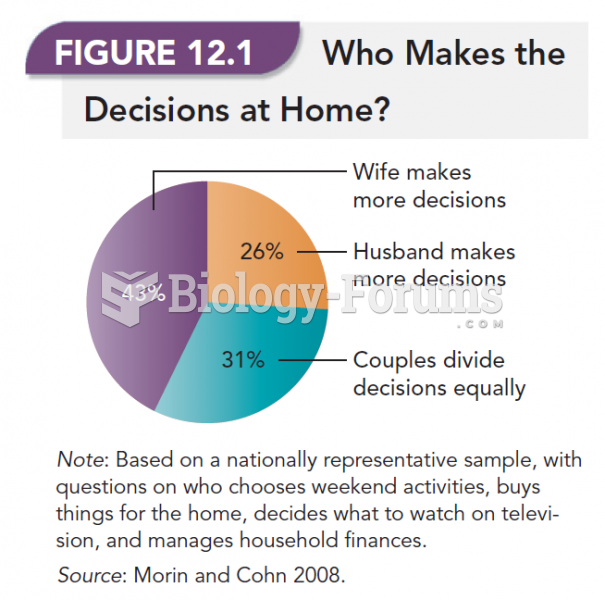 Who Makes The Decisions at Home?
Who Makes The Decisions at Home?
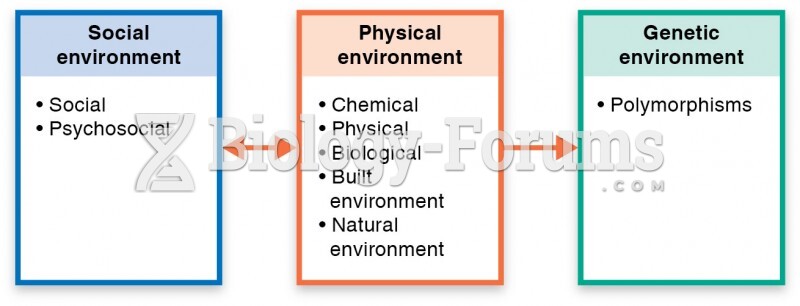 Ecological model for environmental health
Ecological model for environmental health