Answer to Question 1
2
Explanation:
1. The medication must be continued for life.
2. The parents should be cautioned to dress the child appropriately to prevent hypothermia.
3. The infant formula is not contraindicated with the prescribed medication.
4. The child will continue to need monitoring and intervention even if growth and development are not affected.
Answer to Question 2
2
Explanation:
1. Although this nursing diagnosis is applicable, pain is a lower priority than is risk for fluid volume deficit.
2. Adequate fluid volume is a critical physiologic need; therefore, this is the highest-priority nursing diagnosis.
3. Although this nursing diagnosis may be applicable, family coping is a lower priority than is risk for fluid volume deficit.
4. Although this nursing diagnosis may be applicable, a knowledge deficit is a psychosocial issue, and therefore a lower priority than is the physiologic need for adequate fluid volume.

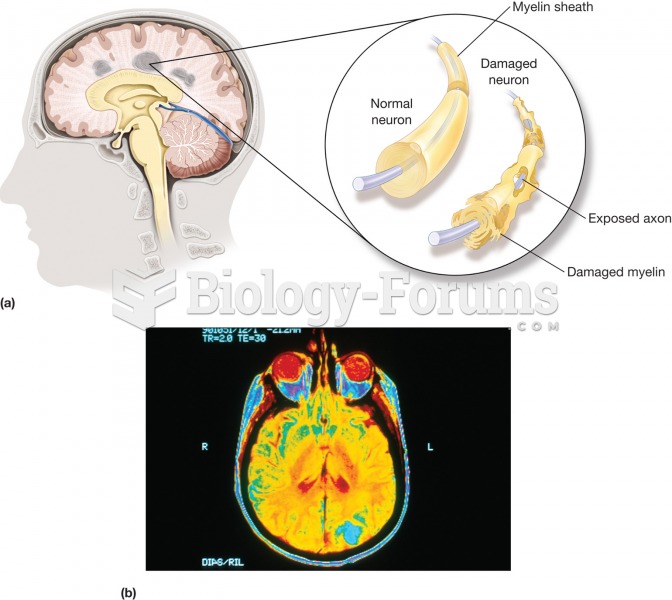 Multiple sclerosis (MS). (a) A disease characterized by the gradual development of small areas of ha
Multiple sclerosis (MS). (a) A disease characterized by the gradual development of small areas of ha
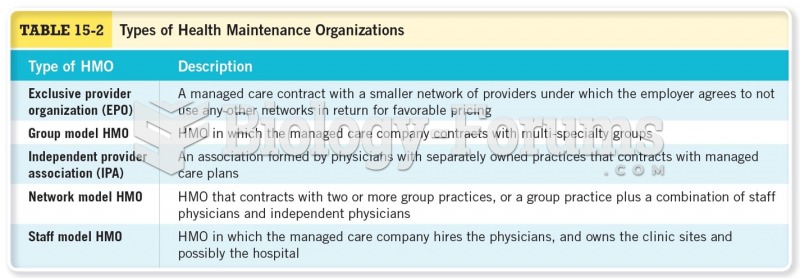 Types of Health Maintenance Organizations
Types of Health Maintenance Organizations
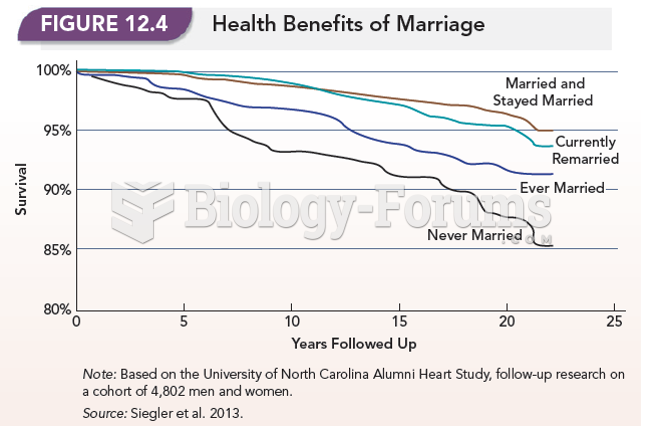 Health Benefits of Marriage
Health Benefits of Marriage
 Old Age and Health
Old Age and Health
 At 19 months, Merr would clearly pass the 17-month item on the Bayley Scales
At 19 months, Merr would clearly pass the 17-month item on the Bayley Scales
 Philip wants to supplement his pension by $415 per month with income from his investments. His ...
Philip wants to supplement his pension by $415 per month with income from his investments. His ...