Answer to Question 1
D
Feedback
A Incorrect. Assessing the accessory (CN XI) and hypoglossal (CN XII) nerves provides clues about the patient's ability to swallow.
B Incorrect. The Confusion Assessment Method is a tool for measuring delirium in intubated or nonverbal patients.
C Incorrect. The MMSE is a valid and reliable tool to assess cognitive function; however, it is unable to pinpoint discreet areas of neurological dysfunction.
D Correct. The nurse uses the Controlled Word Association Test to assess for a neurological cause of this older adult's cognitive dysfunction. This tool is an index of frontal lobe functioning and an assessment of executive function in-cluding the patient's frontal lobe functioning and the ability to refrain from dis-traction and perseveration.
Answer to Question 2
B
Feedback
A Incorrect. Because the patient is intubated and on mechanical ventilation, the nurse cannot apply the MMSE to this patient because the patient is unable to perform adequately. Besides, assessing for dementia is not a prophylactic meas-ure.
B Correct. Providing uninterrupted periods of rest and sleep is a challenge for the nurse in intensive care. Because of the nature of the patients' illnesses, nurses administer medication and treatments and perform invasive procedures on a 24-hour basis, leaving the patient little time for rest. Many patients become deli-rious in the intensive care unit because the noise, activity, brightness, and dis-turbance tend to persist around the clock. This contributes to delirium as the pa-tient loses sources for maintaining orientation and stability; that is, bright light-ing at all times leading to disruption in the circadian rhythm and unfamiliar, ab-rupt increases in noise. In addition, patients in intensive care are more likely to receive multiple medications and medications that are potentially harmful and can aggravate the patient's cognitive difficulties.
C Incorrect. Sedation and pain management, although often needed in the inten-sive care unit, can contribute to delirium.
D Incorrect. Covering the eyes of a patient in intensive care with ointment can be necessary to prevent corneal damage; however, it is likely to contribute to deli-rium because the patient will be unable to see clearly.

 These young adults look forward to a life together as they celebrate their wedding
These young adults look forward to a life together as they celebrate their wedding
 Nurse Sandy
Nurse Sandy
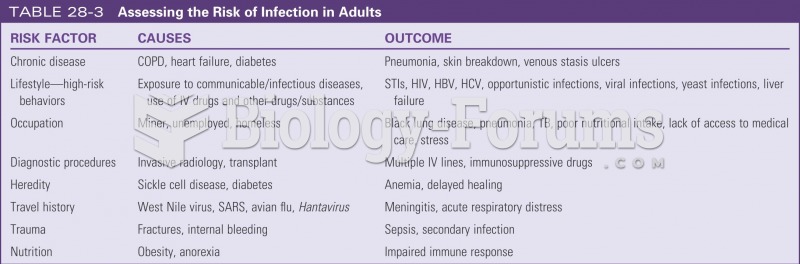 Assessing risk for infection in adults
Assessing risk for infection in adults
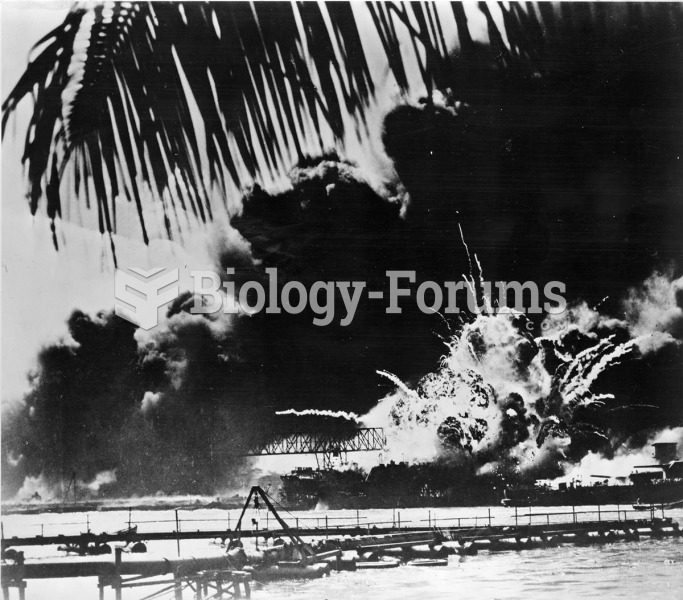 Japan’s surprise attack on Pearl Harbor on December 7, 1941, killed more than 2,400 American ...
Japan’s surprise attack on Pearl Harbor on December 7, 1941, killed more than 2,400 American ...
 In many industrialized nations, men are having children at older ages, raising the possibility of ...
In many industrialized nations, men are having children at older ages, raising the possibility of ...