This topic contains a solution. Click here to go to the answer
|
|
|

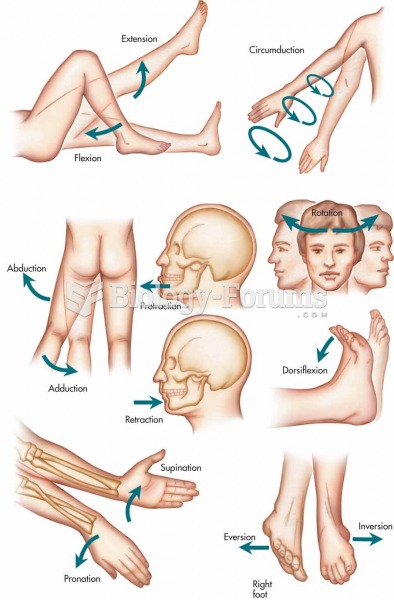 The following terms describe types of body movement that occur at the diarthrotic joints
The following terms describe types of body movement that occur at the diarthrotic joints
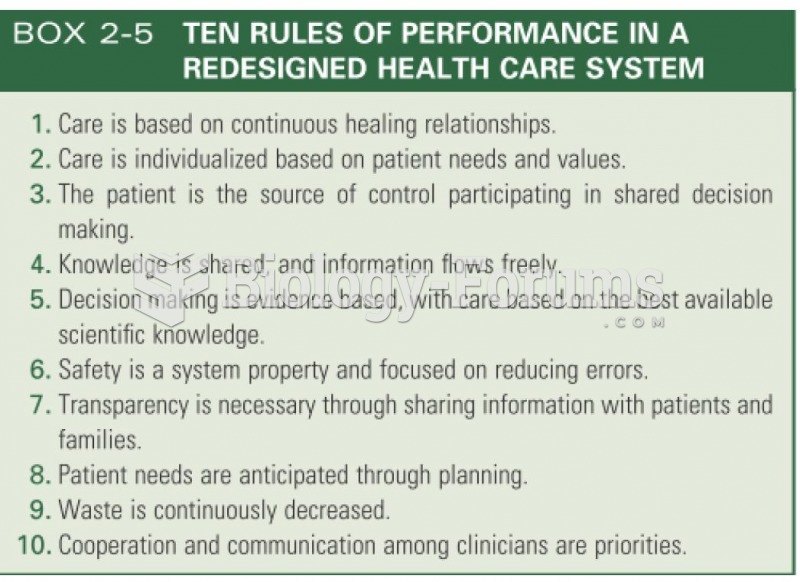 TEN RULES OF PERFORMANCE IN A REDESIGNED HEALTH CARE SYSTEM
TEN RULES OF PERFORMANCE IN A REDESIGNED HEALTH CARE SYSTEM
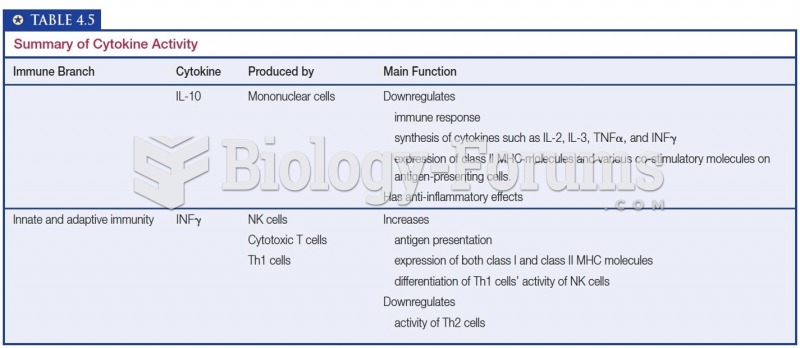 Summary of Cytokine Activity
Summary of Cytokine Activity
 How to describe transformations of a sinusoidal function (y=a*sinb(x−c)+d)
How to describe transformations of a sinusoidal function (y=a*sinb(x−c)+d)
 DDT impact on human health
DDT impact on human health
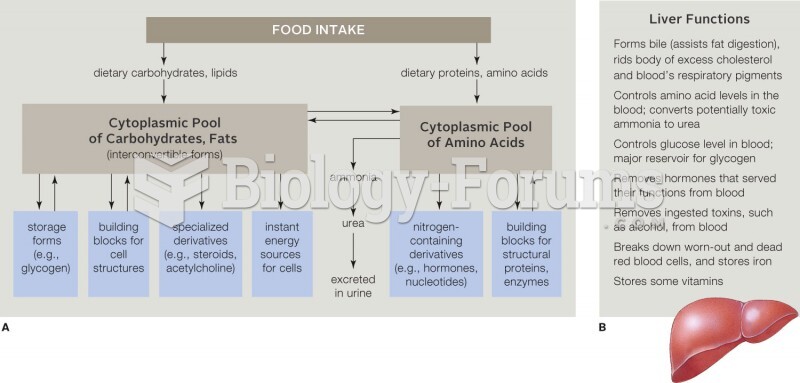 (a) Summary of major pathways of organic metabolism. Cells continually synthesize and break down car
(a) Summary of major pathways of organic metabolism. Cells continually synthesize and break down car