Answer to Question 1
ANS: B
If a leak is present during a positive-pressure breath, air can be heard escaping from the patient's mouth. If there is a large enough leak, the ventilator's low-pressure and low-volume alarms will sound. A circuit leak or disconnection would cause the low alarms to sound but not cause the leak around the endotracheal tube cuff. An incorrect endotracheal tube may cause a leak around the cuff. However, a size 7 mm ID is appropriate for this particular size patient.
Answer to Question 2
ANS: B
Late inspiratory crackles and infiltrates on the chest X-ray are indicative of consolidation due to pneumonia. A patient having an asthma exacerbation would present with wheezing, hyperreso-nance on percussion, and increased radiolucency on X-ray. A patient with a pneumothorax would have unilateral absence of breath sounds, hyperresonance on percussion over the affected area, and lack of vascular markings over the affected area on X-ray. A pleural effusion manifests itself on X-ray as a blunting of the costophrenic angle on the affected side, a pleural friction rub just above the fluid level, and dullness to percussion over the pleural effusion.

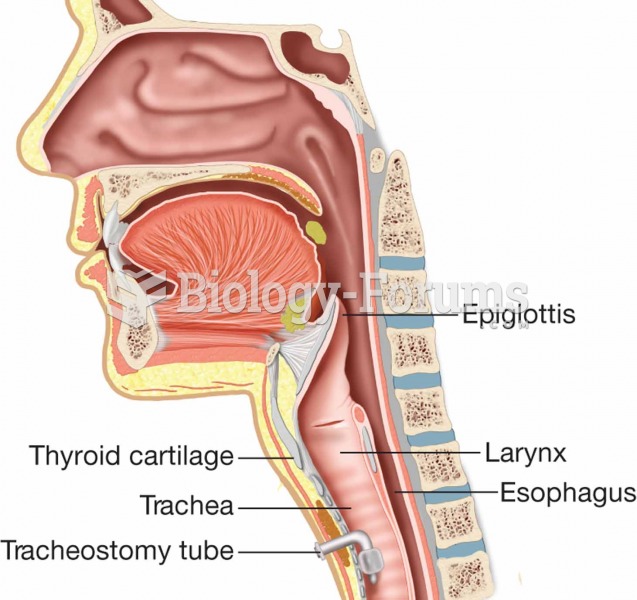 Tracheostomy tube in place.
Tracheostomy tube in place.
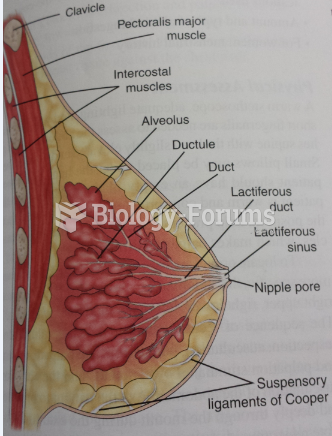 Female Breast
Female Breast
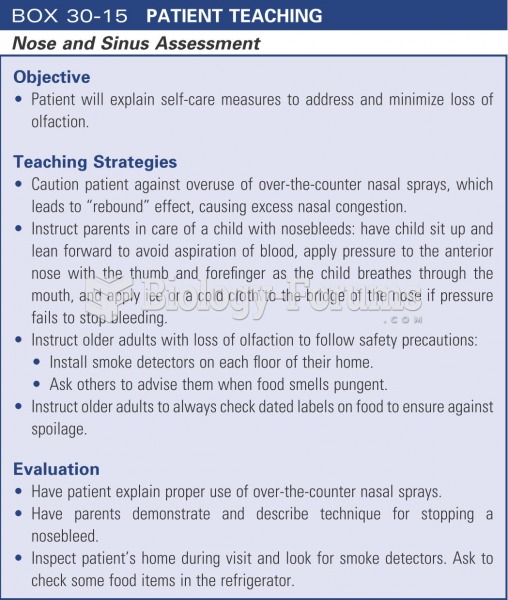 Patient teaching: nose and sinus assessment
Patient teaching: nose and sinus assessment
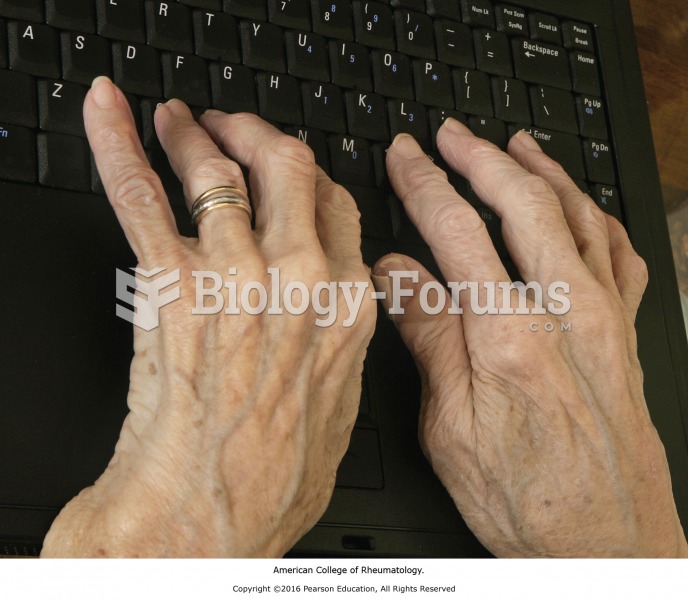 Patient with rheumatoid arthritis.
Patient with rheumatoid arthritis.
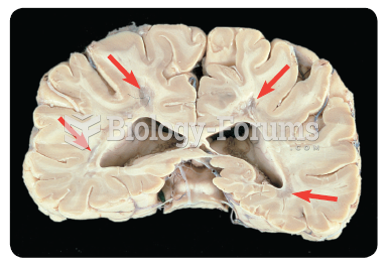 Areas of sclerosis (see arrows) in the white matter of a patient with MS.
Areas of sclerosis (see arrows) in the white matter of a patient with MS.
 If the following ions Ca2+, Cl-, Na+ and CO32- are placed in a test tube, the precipitate ...
If the following ions Ca2+, Cl-, Na+ and CO32- are placed in a test tube, the precipitate ...