This topic contains a solution. Click here to go to the answer
|
|
|

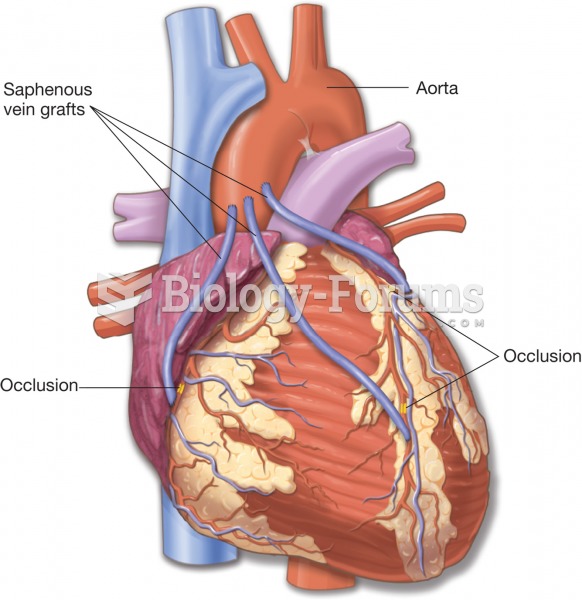 Coronary artery bypass graft (CABG). The grafts are often obtained from the patient’s saphenous vein
Coronary artery bypass graft (CABG). The grafts are often obtained from the patient’s saphenous vein
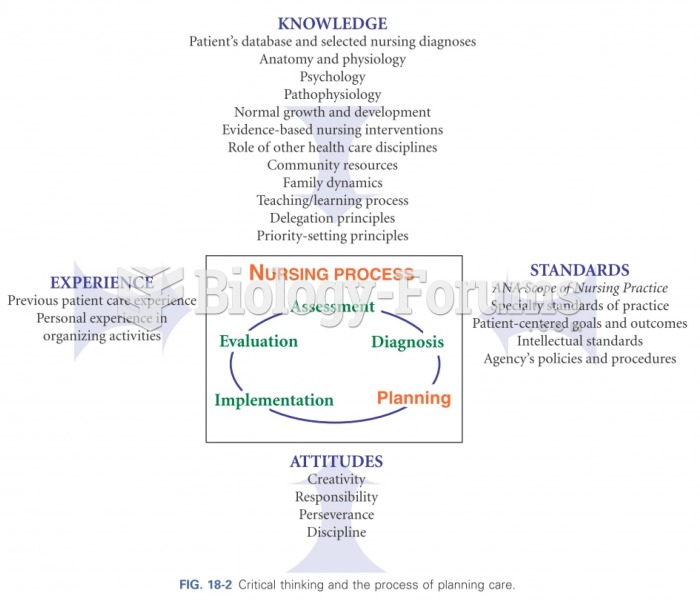 Critical thinking and the process of planning care
Critical thinking and the process of planning care
 A medical assistant helps the physician with a patient.
A medical assistant helps the physician with a patient.
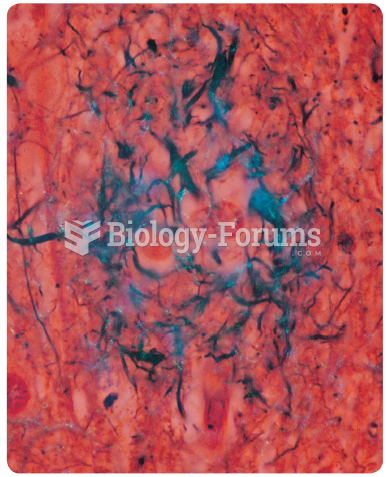 Amyloid plaques (stained blue) in the brain of a deceased patient who had Alzheimer’s disease.
Amyloid plaques (stained blue) in the brain of a deceased patient who had Alzheimer’s disease.
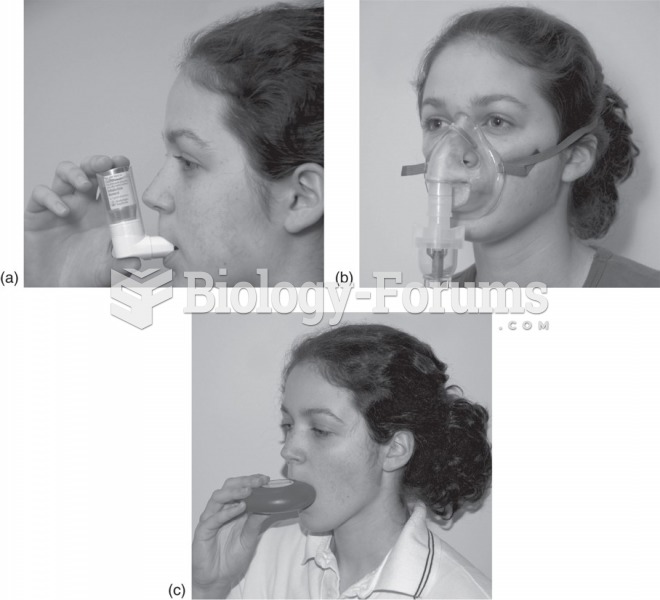 Inhalers used to deliver asthmatic drugs: (a) Metered-dose inhaler. The patient times the inhalation ...
Inhalers used to deliver asthmatic drugs: (a) Metered-dose inhaler. The patient times the inhalation ...
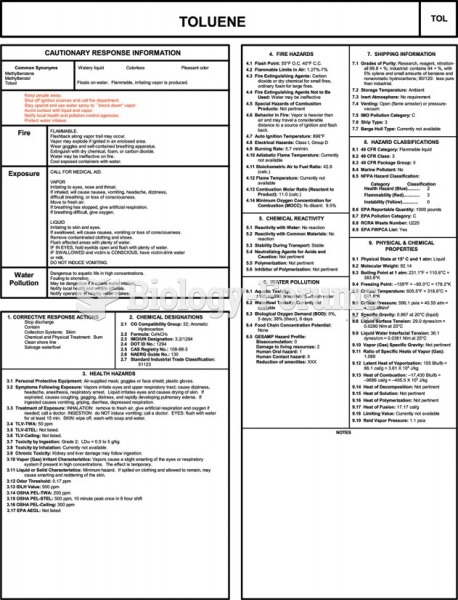 The CHRIS manual entry for toluene. Useful information includes response information, chemical and ...
The CHRIS manual entry for toluene. Useful information includes response information, chemical and ...